Introduction
Hip osteoarthritis or coxarthrosis is very disabling in its advanced stages(1,2). The underlying cause of coxarthrosis has not been fully established. However, in 2003, Ganz et al. described femoroacetabular impingement (FAI) as one of the factors predisposing to coxarthrosis(3).
Femoroacetabular impingement is a disease condition resulting from a pincer-type morphology of the acetabulum or from a cam-type morphology of the femoral head and neck. This, combined with specific kinematics, produces biomechanical alterations that lead to coxarthrosis(4,5,6). Although a logical relationship has been established between FAI and coxarthrosis, particularly in cam-type lesions, this is not always so. Likewise, from the clinical perspective, some patients with FAI-type anatomical alterations in the imaging studies are seen to be asymptomatic(7). The development of arthroscopic techniques in general and research into the association between FAI and coxarthrosis have favoured the use of hip-preserving surgical procedures such as arthroscopy(8).
At present, arthroscopic hip surgery (AHS) is commonly performed in departments of orthopaedic surgery(9). Hip arthroscopy has been shown to adequately correct FAI, with few complications and relatively short recovery periods, and is seen to afford very satisfactory outcomes over the short and middle term(10,11,12,13,14). In view of the notion that FAI predisposes to coxarthrosis, and as a result of improved understanding of the syndrome, the number of patients diagnosed with FAI and the number of hip arthroscopies have increased rapidly in the last few decades(15,16). In our Department, the hip surgeons have been performing AHS for over 10 years. The present study was thus carried out to compare the evolution over time of the indications of AHS referred to the diagnosis of FAI and the evolution of the number of indications of total hip arthroplasty (THA) referred to a diagnosis of primary or idiopathic coxarthrosis in patients under 60 years of age. The study hypothesis was that in this time period, with the incorporation of AHS, the number of indications of THA has decreased.
Material and methods
A retrospective, longitudinal, single-centre observational study was carried out. The trial was conducted in the Department of Orthopaedic Surgery and Traumatology of a tertiary hospital of the Spanish public healthcare system between January 2009 and December 2015. The patients were identified from our orthopaedic surgery registry. The study was evaluated and approved by the Ethics Committee with reference 2016_25 (ARTROS2016). The inclusion and exclusion criteria were evaluated based on the information contained in the electronic health records system.
The patients were included in the statistical analysis if they met all the following inclusion criteria: 1) patients between 18-60 years of age at the time of surgery; and 2) patients subjected to elective hip surgery during the period between January 2009 and December 2015 due to FAI (International Classification of Diseases - Ninth Revision [ICD-9] code: 718.85) or primary or idiopathic coxarthrosis (ICD-9: 715.9). A review was made of the surgical waiting list and of the surgical sheets of all the patients between 18-60 years of age (1260 surgeries) in order to identify individuals operated upon by the Hip Unit of our Department, with FAI and coxarthrosis, subjected to surgery with other codes, or who had been wrongly coded. The exclusion criteria were: 1) patients subjected to primary hip arthroscopy for other reasons, such as diagnostic arthroscopy, intraarticular free bodies, etc.; 2) patients subjected to THA for other reasons such as prosthetic revision surgery, fractures, avascular necrosis, etc.; and 3) patients presenting an incomplete case history, with a missing surgical sheet (7 patients).
Statistical analysis
Categorical variables were reported as absolute frequencies and percentages. Quantitative variables were reported using measures of central tendency: mean, median and standard deviation (SD). The trend in the number of both surgeries during the follow-up period (7 years) was evaluated using the Pearson correlation coefficient with the corresponding 95% confidence interval (p < 0.05). The statistical analysis was performed using the Stata version 23.0 package (StataCorp, Texas, USA).
Results
Of the 1260 reviewed surgeries, 5.6% (70 patients) presented coding errors, i.e. they corresponded to other diagnoses that had been wrongly coded as FAI. Likewise, 22.9% surgeries (289 patients) presented other diagnoses that had been erroneously coded as primary THA.
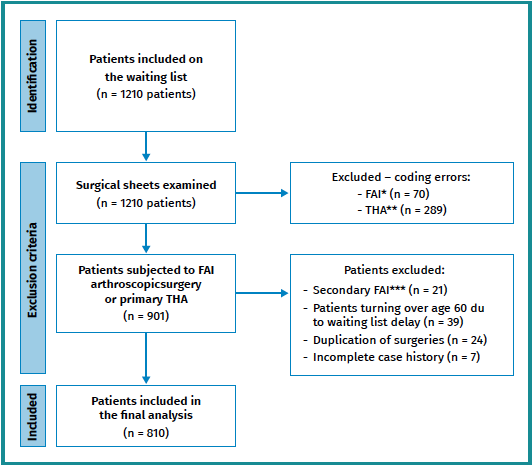
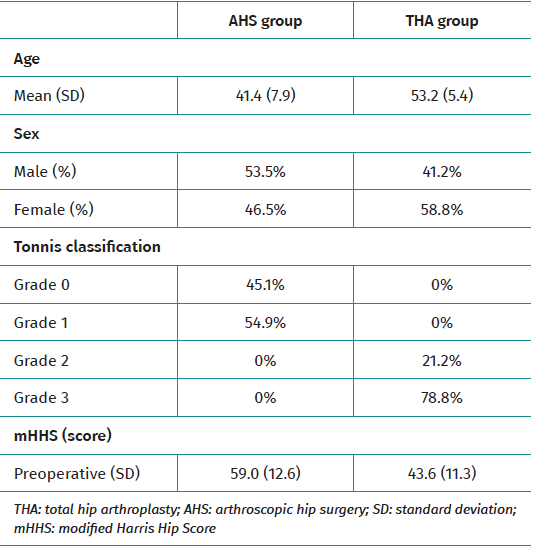
In the period between January 2009 and December 2015, the surgical waiting list reviewed by means of the surgical sheets included 810 patients subjected to AHS due to FAI and primary THA secondary to primary or idiopathic coxarthrosis between 18-60 years of age (Figure 1). Of this total, 288 patients corresponded to AHS due to FAI (35.6%) and 522 to THA secondary to primary or idiopathic coxarthrosis (64.4%). Table 1 shows the demographic data of both groups.
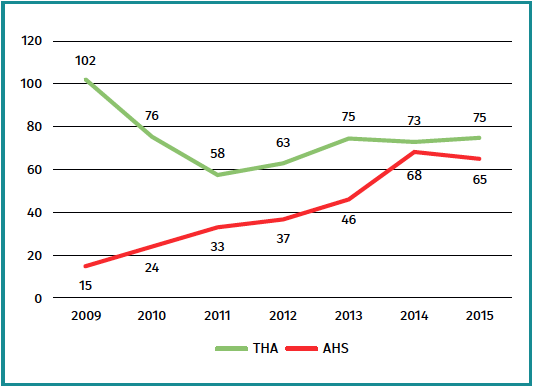
An increase of 433.3% was observed in the number of AHS due to FAI between 2009 and 2015, while the indication of primary THA decreased 26.5% in the same time period, in patients under 60 years of age (Figure 2). The indications referred to THA decreased as the indications of AHS increased, almost becoming equal in 2014. The AHS cohort showed a significant increasing trend, while the THA cohort showed a significant decreasing trend in the number of procedures performed during the mentioned 7-year period (p < 0.001).
Discussion
The main finding of the present study was that the increase in indications of hip arthroscopy due to FAI was associated to a decrease in the indications of primary THA, with a clear change in the trend in patients under 60 years of age. The two procedures were almost equalised in 2014.
We observed a tendency towards increased indication of hip arthroscopy due to FAI between 2009 and 2015. A 433.3% increment was recorded between 2009 and 2015. This tendency to increase has also been seen in other studies(16,17). Montgomery et al. reported a 365% increase in the hip arthroscopy rate between 2004 and 2009 in their cohort of patients in the United States. Zusmanovich et al. in turn found the incidence of hip arthroscopy in patients with FAI syndrome and disease of the labrum to increase 85% in the period 2011-2018 in the United States(17).
Likewise, a decrease in the incidence of primary THA of 26.5% was observed between 2009 and 2015. These data indicate a rising trend in hip arthroscopic treatment as a management approach to patients under 60 years of age with coxalgia and the absence of advanced joint degeneration (Tonnis grades I-II). From this same perspective, hip joint preservation surgery, i.e. surgery seeking to delay or avoid the appearance of hip arthrosis, has experienced an increase in the last decade(1,2,18,19,20). This is reflected in the change in trend at our centre, with hip arthroscopy being the treatment of choice for patients with FAI.
The increase in hip arthroscopy is probably due to a number of factors. These factors include surgical technical advances, improved diagnostic techniques, the expansion of indications, and increased emphasis on hip arthroscopy in resident training programmes and training scholarships(15,16,17). It has not yet been established whether this increase in hip arthroscopy results in a decrease in the number of hip prosthetic implants, however. Kowlaczuk et al., in a systematic review, concluded that FAI contributes to the development and progression of hip arthrosis(19). Once it is accepted that FAI can eventually lead to osteoarthritis of the hip, the other major remaining question is whether "prophylactic" surgery (in asymptomatic patients) is indicated. In this regard, two reviews concluded that prophylactic surgery is not indicated, since it could be regarded as unnecessary in up to 80% of all cases(20,21). It is important to mention that despite the associations observed between FAI and coxarthrosis, most patients with radiographic FAI do not develop degenerative changes and will not require THA(19,22).
The present study has limitations, such as its retrospective design and limited number of patients. In addition, a description of the patient characteristics is lacking in the global number of surgeries. In this study we have observed a tendency towards an increased indication of hip arthroscopy in a University hospital. The literature offers no specific articles addressing changes in trend in indication or increases in the indication of hip arthroscopy versus THA. It would be interesting to conduct studies with a longer follow-up to establish the half-life of surgical success (defined as no need for further surgery), and to identify the underlying influencing factors and investigate whether they could be modified. Likewise, we wish to underscore that although there has been an increase in the indication of AHS, it cannot be affirmed that this increase has induced a decrease in the indication of THA.
Conclusion
There has been a significant increase in the use of hip arthroscopy for the treatment of FAI at our centre. Based on these results, we have observed an increase in the indication of conservative arthroscopic hip surgery and a decrease in the indication of THA at our centre, though no cause-effect relationship can be established.


