Introduction
The elbow is the second most common joint to suffer dislocation in adults(1), representing 10-25% of all elbow injuries. Most such dislocations occur in the posterolateral or posterior direction(2).
The majority of posterior elbow luxations occur as a result of falls with the elbow in extension, through an axial compression mechanism, with the forearm in supination and valgus, giving rise to soft tissue injury that progresses in a circular manner from lateral to medial. Posterolateral rotary instability, described by O'Driscoll et al. in 1991(3), is the most common presentation following posterior elbow dislocation that has failed to respond to conservative management, and occurs due to damage to the lateral ligament complex, which is in charge of limiting external rotation of the radius and ulna with respect to the humerus, in addition to varus stress.
The by now chronic damage to the lateral collateral ligament can be resolved by means of a plasty procedure (Docking or Gong type)(4,5,6). Another option is a dynamic internal fixation system (IJS® Elbow) from Skeletal Dynamics(7,8), which is indicated for temporary use in chronic instability.
In addition, posterior elbow luxation may also involve chondral damage secondary to impingement of the radial head against the capitellum. These osteochondral defects, referred to as Osborne-Cotterill lesions, are a cause of pain and residual instability if not treated along with the rest of the elbow lesions.
We present the case of a woman with posterolateral rotary instability of the right elbow who also presented an osteochondral defect of the capitellum (Osborne-Cotterill lesion).
Clinical case
A 53-year-old woman with no relevant personal history suffered a fall with trauma of the right elbow and ankle. The patient described the fall as occurring with the shoulder raised and the elbow extended and in supination. She suffered functional impairment of the elbow, with posterior deformity of the latter. In the emergency service and following physical examination and radiographs, the patient was diagnosed with posterior dislocation of the elbow with impact fracture in the posterior region of the lateral condyle, in addition to subtalar luxation. The elbow dislocation was reduced that same day, exerting downward traction over the forearm with the elbow in 90º flexion, and with immobilisation by means of a posterior arm splint. After three weeks the patient was examined in the outpatient clinic and the splint was removed. She then started 8 weeks of rehabilitation, with a rapid gain of joint balance (0-120º).
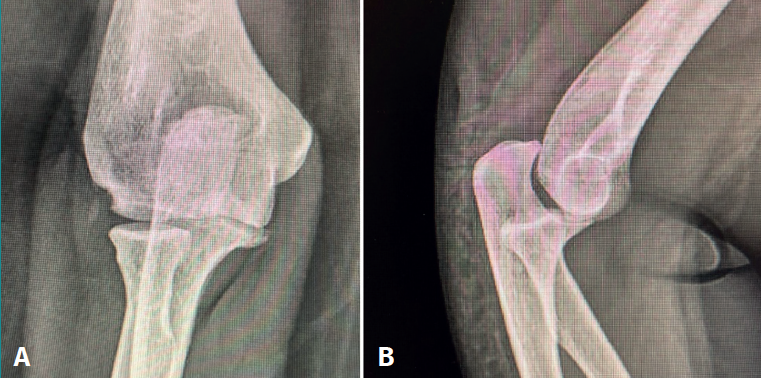
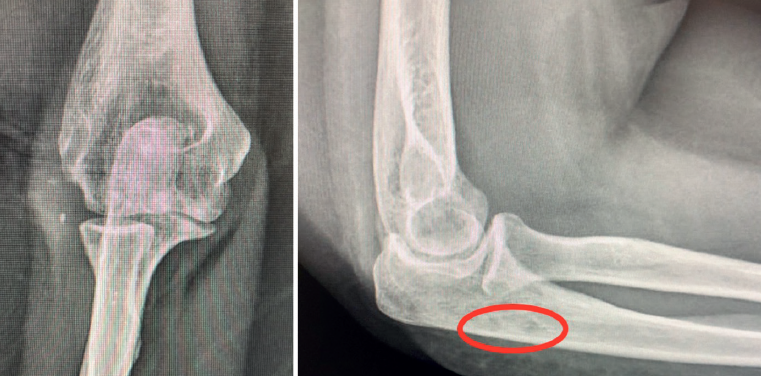
The patient was again evaluated in the clinic after 12 weeks. The physical examination revealed pain on the lateral aspect of the right elbow, with clicks on pronation, positive pivot shift manoeuvre and painful varus laxity. Complementary tests were requested: radiographs, which evidenced the Osborne-Cotterill lesion (Figure 1); a magnetic resonance imaging (MRI) scan showing distal deinsertion of the ulnar lateral collateral ligament and proximal deinsertion of the radial collateral ligament, as well as partial rupture of the annular ligament; and a computed tomography (CT) scan that found the Osborne-Cotterill osteochondral defect in the posterior capitellum to measure 8 × 3 mm (Figure 2). The patient suffered another posterior dislocation episode the following week after a new fall while undergoing rehabilitation. A second closed reduction was therefore performed.

In total, she experienced three further subluxation episodes in these weeks. In view of the great instability, surgical treatment was decided 6 months after the initial injury. The operation consisted of Docking type ligamentoplasty with an autologous graft from the gracilis muscle of the right knee and mosaicplasty measuring 8.5 mm in diameter with autologous grafting from the same knee.
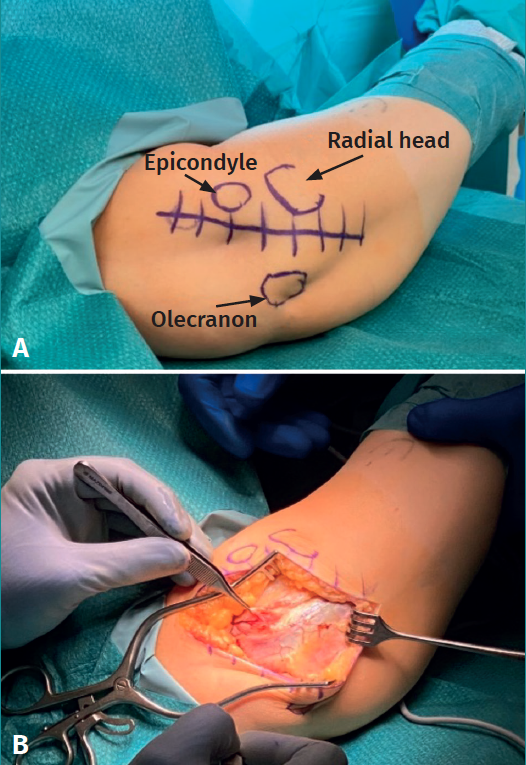
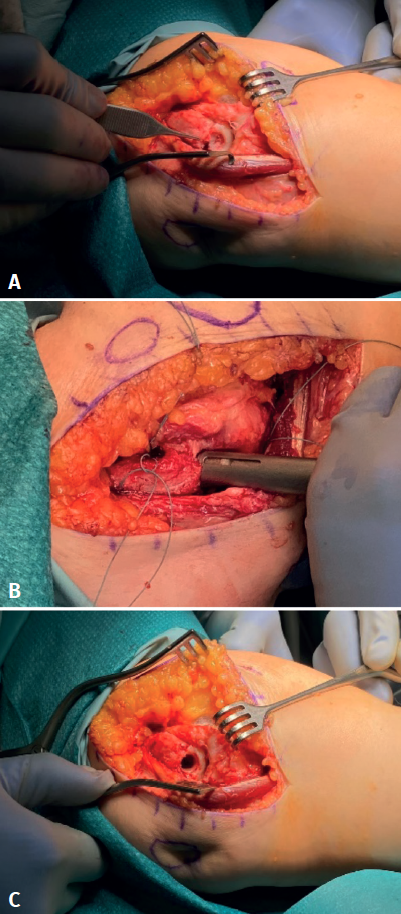
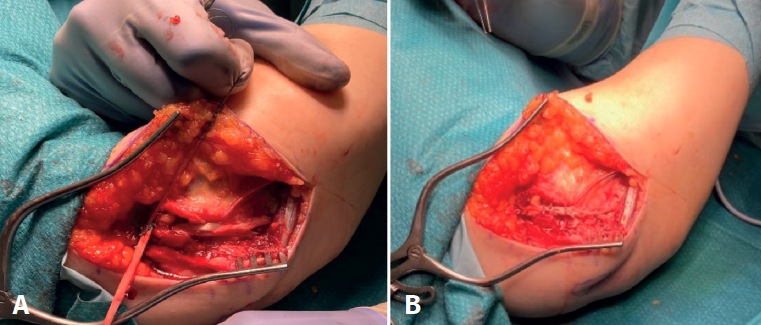
With the patient in supine decubitus, and following general anaesthesia with ischemia of the root of the right arm, a 5-cm longitudinal incision was made over the lateral column of the humerus (Figure 3A) with a Kocher approach between the anconeus and extensor carpi ulnaris (Figure 3B), raising the anconeus from the ulna until exposing the posterior part of the joint. The bone bed in the receptor zone (capitellum) measured 8 mm in diameter and 3 mm in depth (Figure 4A). This bed was prepared for the mosaicplasty (Figures 4B and 4C).
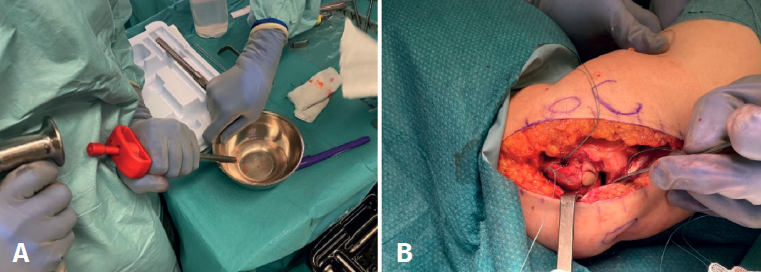
The osteochondral graft was then harvested. It was obtained from the lateral femoral trochlea, as this is not a weight-bearing zone, and thus constitutes a good bone and cartilage donor site. The Mosaicplasty® system of Smith & Nephew was used for this purpose, through an open arthrotomy measuring about 2 cm, yielding an 8.5-mm cylinder (Figure 5A) that was impacted in the prepared receptor zone (Figure 5B).
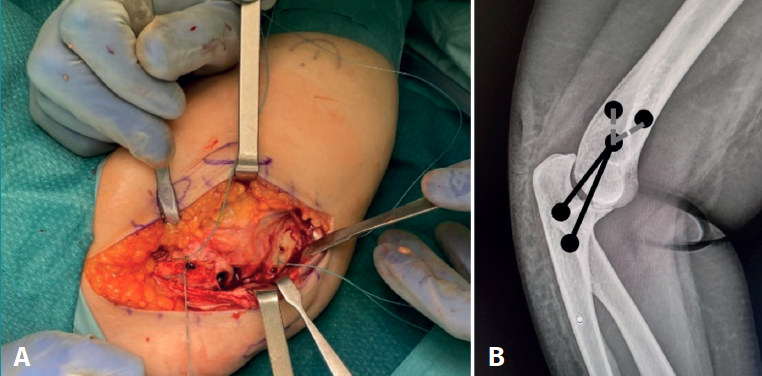
The ulnar tunnels for passing the tendon graft were required to be convergent and measured 3.5 mm in diameter, and were made following the introduction of Kirschner pins with the use of cannulated drills (Figures 6A and 6B): the more distal at the level of the supinator crest and the proximal at the level of the insertion of the annular ligament, taking care to leave a 1.5-cm bone bridge between them. The humeral tunnels presented a "Y" configuration. The more distal tunnel measured 4.5 mm and was made at the isometric point, while the other two (one anterior and the other posterior) measured 3.5 mm in diameter and were located more proximal and convergent to the first tunnel.
The plasty was prepared with Krackow sutures at the extremities, and suture loops were left in the tunnels to serve as transporters.

Once the plasty was passed through the ulnar tunnels, its extremities were crossed and both were inserted through the distal humeral tunnel, with each extremity emerging from one of the proximal orifices (Figure 7).
At this point the extremities were joined using Ethibond suture with the elbow flexed 40º and in pronation, leaving the plasty in an extraarticular position (Figures 8A and 8B).

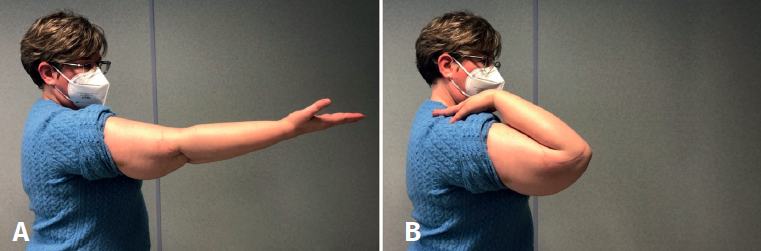
Following an immediate postoperative period (Figure 9) without complications and with adequate rehabilitation, the patient has been able to return to her normal life four and a half months after surgery. Upon exploration, the elbow proved stable, with a full joint motion range, and the patient was able to perform axial loading without pain or failure sensation (Figures 10A and 10B). The radiographs evidenced the reduced elbow (Figure 11).
Discussion
Chronic posterior dislocation of the elbow requiring surgical treatment, as in our case, is an infrequent condition. This combined lesion (osteochondral defect of the capitellum and damage to the lateral collateral ligament [LCL]) was resolved by mosaicplasty and Docking ligamentoplasty, with a good postoperative outcome. Good understanding of the characteristics of the lesion (i.e., direction of the luxation, soft tissue lesion features and stability after reduction) is important for deciding the most effective treatment in such cases.
The ligaments enveloping the lateral capsule of the elbow are the LCL or radial ligament, the ulnar LCL (ULCL), the accessory LCL and the annular ligament. In addition to stabilising the lateral aspect of the elbow, the ULCL acts as a posterior stop for the radial head, avoiding its subluxation(9). On flexing the elbow, damage to the ULCL causes the ulna to undergo anomalous supination over the humerus, with posterior and lateral subluxation of the radial head, associated to both ulnar and radial displacement in external rotation and valgus.
In isolated luxation of the radial head, the proximal radioulnar joint ruptures, while the humeroulnar joint remains intact. In contrast, in posterolateral rotary instability, the proximal radioulnar joint is preserved and the two bones of the forearm rotate as a single unit(10).
According to Horii(11), the pathophysiology of elbow instability can be explained by considering that the joint is a circle that ruptures in three stages. Stage 1 is characterised by ULCL rupture, producing posterolateral subluxation of the radial head upon supination of the elbow. If the lesion progresses medially, the anterior capsule and posterior capsule of the elbow rupture; the humeroulnar joint experiences subluxation, and the coronoid process becomes trapped in the humeral trochlea (stage 2). If the force progresses, the elbow suffers complete dislocation(12). This last stage in turn is divided into substage 3a, characterised by soft tissue involvement, except for the anterior band of the medial collateral ligament. In substage 3b the anterior band also ruptures, leaving the elbow unstable in valgus. Lastly, in substage 3c, the elbow is completely unstable multi-directionally. This model of the circle of Horii is analogous to the perilunar instability pattern of Mayfield seen in the wrist(13).
Posterolateral rotary instability occurs as a result of damage to the lateral ligament complex of the elbow following trauma-induced dislocation combining axial compression + supination + valgus over the elbow(14). Such posterolateral instability occurs in less than 10% of all cases of elbow dislocation(12). Following a first elbow dislocation episode, conservative management(15) with two weeks of sling immobilisation followed by early rehabilitation usually proves effective(16,17). However, early subluxation or recurrent luxation, as in our case, indicates a lack of healing of the lateral ligament complex, and the manifestation of mechanical pain and varus laxity (on reaching half of the range of extension with the forearm in supination) suggests posterolateral rotary instability, pointing to the advisability of surgical treatment(14).
Reconstruction of the ligament should be anatomical, isometric and extracapsular(12). The most common practice is to recreate the ULCL via a ligamentoplasty with an autologous or heterologous tendon graft that is usually tunnelled and sutured onto itself - location of the isometric point in the humerus being a critical point of surgery. This is done with the elbow flexed and in full pronation(10). It is not always necessary to repair the medial collateral complex, because the elbow may be stable after repairing the LCL complex and extensor musculature, as in our case. The Kocher or posterolateral approach was used in surgery. Consideration is required of possible damage to the posterior interosseous nerve, which can be avoided through pronation of the forearm(2).
Damage to the capitellum secondary to elbow dislocation may go unnoticed on plain X-rays. In this respect, MRI or CT, with a strong clinical suspicion, are needed to establish the diagnosis. Hyojune Kim et al. (2020) found osteochondral lesions in 48.8% of their cases, using MRI, in patients that had suffered simple elbow luxation. Most of these lesions were observed in the posterolateral region of the capitellum(18). However, it is not common to identify an osteochondral defect as large as that seen in our patient, which measured 8 × 3 mm in the posterior region of the capitellum.
Mosaicplasty with autologous osteochondral grafting has been well described in defects of the knee, hip and ankle(19,20), though it has been little mentioned in the elbow(21,22). In contrast, the reconstruction of defects of the coronoid process using radial head autologous grafts has been widely described at elbow level(23,24,25). The capitellum defects described in the literature refer fundamentally to osteochondritis dissecans in young patients and athletes(26). Yamaga et al. (2018) reported good clinical outcomes after covering osteochondral defects of the capitellum in two patients using autologous grafts from the knee(27). Resolution with femoral trochlea grafts is a valid alternative which we considered in this case as a viable treatment option.
Conclusion
Posterolateral rotary instability after conservative management of posterior dislocation is not a common condition in clinical practice. Plasty surgery to reconstruct the lateral complex, in addition to the use of osteochondral grafts to repair joint defects, is a valid option that proves technically demanding from the surgical perspective but affords good long-term outcomes for the patient.










