Introduction
Rotator cuff disease is the most common cause of disability and the most prevalent condition seen in the clinical practice of shoulder surgeons(1). The overall incidence of rotator cuff rupture is between 5-40%(2), and among these injuries there are a significant number of massive ruptures (estimated at about 20%), as well as an important percentage of repeat ruptures (80%)(3). A distinction must be made between massive ruptures and irreparable ruptures, since the former are not necessarily irreparable. Massive ruptures are defined as ruptures presenting a size of > 5 cm in the coronal plane or which affect two or more tendons(4). The definition of irreparable rupture is more controversial. Although massive ruptures can be repaired, the failure rate is 25-94%, depending on the cases, over a follow-up period of two years, and is typically associated with biological failure of the tendon-bone junction(5). Thus, the identification and management of irreparable rotator cuff ruptures constitutes a challenge for surgeons in relation to cost-economical aspects and as regards the short and long term benefits for the patient(6).
Conservative management should be the first line option in ruptures of this kind, and may prove effective in some patients, despite progression of the size of the rupture, adipose infiltration and arthropathy(7). Conservative management includes physical therapy with muscle strengthening and re-education, supported by rehabilitation therapy, oral medication (nonsteroidal antiinflammatory drugs [NSAIDs]) and subacromial infiltrations of corticosteroids, hyaluronic acid (HA) and biological therapies (platelet rich plasma [PRP]). When initial conservative management fails, or in some cases where surgical options are contraindicated because of the age of the patient, failed previous surgeries or the impossibility of repairing the rotator cuff due to the characteristics of rupture, we have new alternatives that are increasingly investigated, such as ablative or pulsed radiofrequency (RF), which can also be useful as initial treatment in selected cases.
The present review addresses conservative management with medications, as well as infiltrations and invasive therapies for dealing with pain. It should be mentioned, however, that few studies have reviewed the results of these treatments(7), and most of them involve a combination of several such therapies, since no conservative management protocol has been established to date(8).
Prognostic factors in the conservative management of irreparable rotator cuff ruptures
Most studies define failed conservative management as the appearance or worsening of pain and/or loss of function, requiring surgical treatment. The overall success rate varies from 32-100%(9). Vad et al.(9) found the poorest outcomes to be associated with a decrease in strength in abduction and external rotation < 3/5, muscle atrophy, superior migration of the humeral head, reduction of the passive range of motion, and the evolution of glenohumeral arthropathy. Yian et al.(10) in turn found loss of flexion < 50° to be associated to poorer outcomes and failure of conservative management. Collin et al.(11) observed that failed conservative management was more common in anterior ruptures of the rotator cuff, though in contrast Agout et al.(12), found no correlation between the zone of rupture and treatment success. Yoon et al.(13) found that patients with an intact subscapularis or hypertrophy of the teres minor presented a 57% success rate with conservative management, versus 32% in patients without these characteristics.
Lastly, it is important to mention that conservative management appears to afford poorer outcomes in individuals with chronic symptoms, defined as those with a duration of over 6 months, in reference to both pain and loss of function(14).
Oral medication
As has been mentioned, oral medication should be the first line of treatment, particularly in patients with low functional demands and comorbidities that contraindicate other types of treatment, and in individuals who develop symptoms or worsen following contusion or trauma, without their limitations having an impact upon the basic activities of daily living(15). According to a systematic review of the clinical practice guides(16), it is possible to recommend both NSAIDs and tramadol hydrochloride to treat pain and improve function, as well as hypnotics for the sleep disturbances which some patients may experience.
These treatments, combined with physical and rehabilitation therapy, can help alleviate pain and improve function, but the results persist only over the short term(17).
Corticosteroids
The use of corticosteroid infiltrations in shoulder disease is a very widespread practice. There is agreement that corticosteroids suppress acute inflammation through inhibition of the protein synthesis of proinflammatory products. Likewise, they afford symptoms relief and transient functional improvement in both rotator cuff disease and in other conditions characterized by shoulder pain (adhesive capsulitis, primary arthropathy,etc.)(18), despite their side effects(19) and the negative impact they appear to have upon the tendon(20). According to the American Academy of Orthopedic Surgeons (AAOS), a single injection along with local anesthetic affords short term symptoms relief and improved joint function(21). A systematic Cochrane review(22) on corticosteroid infiltrations concluded that in the case of rotator cuff disease, the literature offers heterogeneous results referred to benefit compared with the use of placebo at four weeks, with benefit ranging from minor to no significant differences (the studies moreover being variable in terms of methodological quality). Likewise, no significant differences were observed on comparing corticosteroids versus oral NSAIDs. Thus, based on these results, it is difficult to draw any conclusions regarding the short and long term benefits of subacromial corticosteroid infiltrations.
Hyaluronic acid
Due to the potential negative effects of the above treatments, in the last two decades HA infiltration has emerged as an alternative for the conservative management of arthropathy(23), though few articles have investigated its effects in application to rotator cuff injuries. Hyaluronic acid has both analgesic and cartilage protecting properties(23). A review(24) including 11 articles related to HA infiltration in rotator cuff disease and involving a total of 1102 patients concluded that such infiltration improves symptoms and function in patients with rotator cuff lesions, with no adverse effects or reactions. It thus may constitute an alternative to the previous therapies, in view of its biochemical and biomechanical properties - though further studies are needed to determine the most effective molecular weight, and define when and in what lesion grades it should be administered.
Another systematic review and meta-analysis(25) related to the conservative management of arthropathy, including 15 and 7 studies, respectively, documented a significant decrease in pain after three and 6 months of follow-up, as well as functional improvement at all the follow-up timepoints. The comparative studies yielded similar results regarding pain relief versus placebo, saline solution or corticosteroids, and a strong placebo effect was observed in intraarticular injection in the shoulder. Here again there is a need for greater quality randomized clinical trials to assess efficacy, optimum dose, molecular weight and administration routes. As a result, no recommendation referred to the use of HA can be established at this time.
Platelet rich plasma
In a way similar to the treatment described above, there has recently been an increased in the interest and use of PRP injections for the conservative management of rotator cuff disease(26). Platelet rich plasma is an autologous blood product containing abundant growth factors and bioactive cytokines that reduce inflammation and facilitate healing, incrementing cell migration and proliferation, and favoring angiogenesis(27,28). However, there is considerable debate regarding its clinical efficacy, and consensus is lacking as to the usefulness of PRP in rotator cuff disease(29). A systematic review of randomized clinical trials on the use of PRP in rotator cuff disease(30) involving control groups suggests that over the short term, PRP might not be of benefit compared with the control therapies (physical exercise, placebo, corticosteroids), in terms of either improved pain perception or functional improvement. Despite this, the use of PRP is growing, and the existing scientific evidence is still inconsistent. Further studies of greater quality are needed, standardizing the type of rupture and its size, the preparation of PRP and the injected dosage.
Invasive therapies. Nerve blocks and radiofrequency
Due to the high prevalence and potential persistence of shoulder pain, the continued development of new treatments for pain in this region is crucial(31). Nerve ablation is an established strategy for the middle to long term alleviation of persistent pain in other joints(32). Considering that there is a large proportion of patients with chronic and refractory shoulder pain, and that many of them are not candidates for surgery, the existence of shoulder neuroablation protocols is considered necessary(33). We therefore need to know the sensory innervation of the shoulder.
Peripheral neuroanatomy of the shoulder
Suprascapular nerve
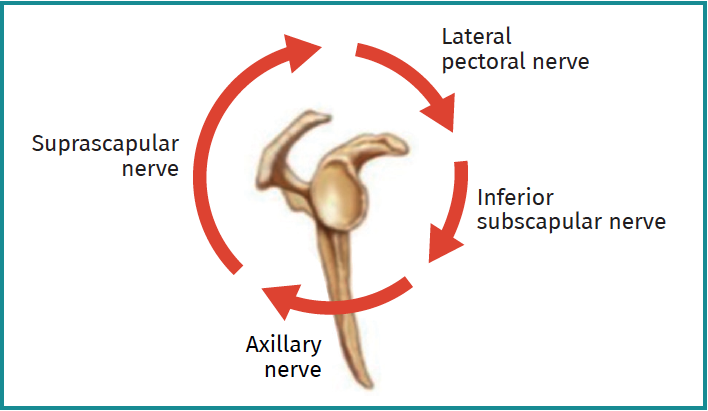
The suprascapular nerve arises from the superior trunk of the brachial plexus. It gives rise to three main articular branches (non-motor): the medial subacromial branch, the lateral subacromial branch and the posterior glenohumeral branch(34). The first branch innervates the coracoclavicular and acromioclavicular ligaments, and the medial portion of the subacromial bursa; the second branch innervates the lateral portion of the subacromial bursa and the acromioclavicular ligaments; and the third branch innervates the posterior capsule of the glenohumeral joint(31)(Figure 1).
Axillary nerve
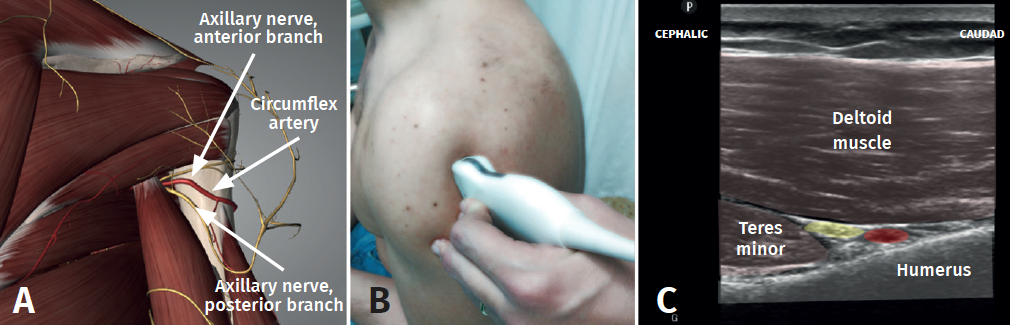
The axillary nerve originates in the posterior fascicle of the brachial plexus. Over its trajectory, the nerve divides into an anterior branch and a posterior branch. On crossing the quadrangular space, the anterior division (which innervates the middle and anterior portion of the deltoid muscle) emits deep articular branches to the tendon of the subscapularis, innervating the anteroinferior capsule(35). Additional branches surround the humerus from posterior to anterolateral, innervating the transverse ligament of the humerus and the tendon of the long head of the biceps. In 60% of the studied specimens, branches from the anterior division run superiorly and in depth to the deltoid muscle to innervate the lateral portion of the subacromial bursa. The posterior division in turn innervates the teres minor and the posterior region of the deltoid muscle, and emits articular branches to the inferior glenohumeral ligament and the posteroinferior capsule(36)(Figure 1).
Lateral pectoral nerve
This nerve arises from the lateral fascicle of the brachial plexus and innervates the greater pectoral muscle (pectoralis major). A sensory portion crosses medial to lateral superficial to the coracoid process. It has been seen that this articular branch crosses more consistently at the midpoint between the tip of the coracoid process and the clavicle. It emerges anterior to the acromioclavicular joint, in the coracoacromial and coracoclavicular ligaments, in the subacromial bursa and in the anterior glenohumeral capsule(37)(Figure 1).
Superior and inferior subscapular nerves
These nerves originate in the posterior fascicle of the brachial plexus, or sometimes from the axillary nerve, respectively. They provide motor innervation for the subscapularis muscle, followed by the emission of submuscular articular branches(38). The superior subscapular nerve innervates the anterosuperior capsule, while the inferior nerve innervates the tendon of the long head of the biceps(39)(Figure 1).
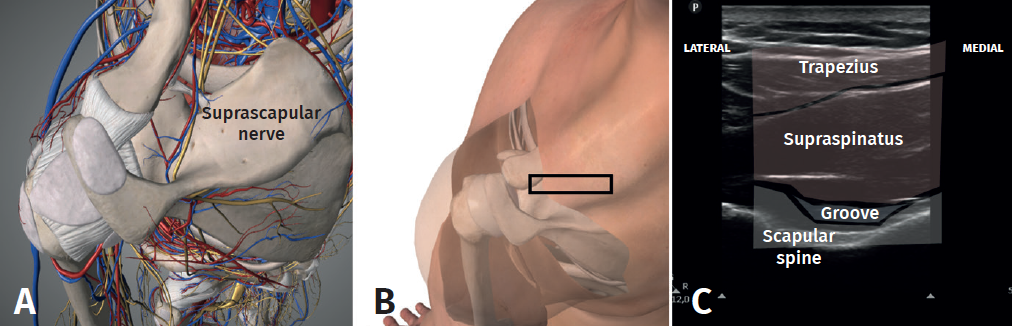
Ablation zones for the treatment of shoulder pain(31)
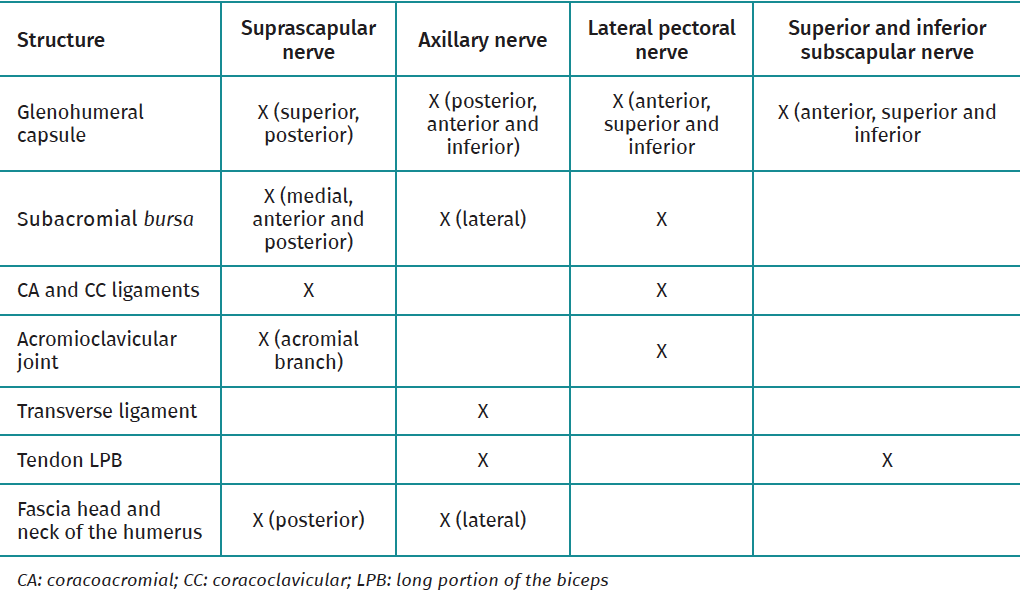
Based on detailed reviews of the zones available for ablation and with current knowledge of the innervation of the shoulder, four potential ablation zones are recommended. However, despite the current use of the technique, further studies and validation are needed. On performing ablation lateral to the supraglenoid groove, at the upper half of the glenoid neck in its posterosuperior region, the subacromial lateral and posterior glenohumeral branches of the suprascapular nerve may be affected, without damaging its motor component (Figure 2). In order to target the subacromial medial branch of the suprascapular nerve, the location must be in the anterosuperior portion of the glenoid neck, near the base of the coracoid process. The ascending branches of the axillary nerve are usually found close to the junction between the posteroinferior margin of the greater tubercle and the metaphysis of the humerus (Figure 3). According to the above description referred to the trajectory of the articular branch of the lateral pectoral nerve, its safe ablation would be in the superficial middle zone of the coracoid process. Motor stimulation must be performed in all these zones in order to avoid damaging the motor fibers. Thus, on performing nerve ablation of the shoulder, we would be carrying out denervation mainly of the following targets: anterosuperior and middle-posterosuperior glenohumeral capsule, subacromial bursa, the coracoacromial and coracoclavicular ligaments, and the acromioclavicular joint (Table 1).
Types of radiofrequency: ablative and pulsed
Ablative radiofrequency is performed at temperatures of 70-80ºC, and results in neuron destruction(40). In application to sensorimotor nerves, ablative radiofrequency may affect motor function. For this reason pulsed radiofrequency began to be used as an alternative, since it involves temperatures of between 40-45ºC, thus avoiding the loss of neuron function but exerting a neuromodulatory effect that contributes to analgesia(41). The procedure usually involves the induction of a prognostic anesthetic block, and if the pain is seen to decrease by over 50%, the corresponding technique is applied. The most commonly used pulsed radiofrequency sequence consists of pulses of 2 Hz spaced 20 ms apart, and with a duration of 2-10 minutes(41).
Results of radiofrequency
Despite the above observations, there is a lack of due evaluation of the results obtained with the two types of radiofrequency treatment in application to the innervation of the shoulder joint. Furthermore, there is considerable variability of the neural targets in radiofrequency procedures.
A systematic review and meta-analysis(42) analyzed the results of these procedures in terms of function, pain improvement and adverse effects, as outcomes of interest. The primary result was the change in pain intensity while the secondary results were referred to function, mobility, strength, disability and patient quality of life or satisfaction. A total of 42 studies were reviewed (36 related to pulsed radiofrequency and 6 to ablative radiofrequency). The origin of the pain included rotator cuff disease and adhesive capsulitis as the two most common diagnoses. Most of the studies were focused on the application of radiofrequency over the suprascapular nerve, with secondary emphasis on the rest of the nerves. On performing a meta-analysis of 7 randomized clinical trials comparing pulsed radiofrequency versus a control group, the evidence was found to be poor, with doubtful results indicating that pulsed radiofrequency affords analgesia and functional improvement versus conventional medical treatment of chronic shoulder pain.
In relation to the review of case series, most of the publications reported a more than 50% decrease in pain with pulsed radiofrequency, with a duration of effect of between days and up to two years. In the case of ablative radiofrequency, all the studies reported a pain intensity reduction of over 50%. The case series on ablative and pulsed radiofrequency also evidenced improvements in function in most studies. There were no important adverse effects. This study highlights the need for new studies focused on other ablation therapeutic targets, scale-based registries, clinical studies evaluating different imaging techniques for performing radiofrequency, and comparative studies of the different ablation techniques.
Conclusions
Many conservative management options are available for irreparable rotator cuff ruptures, though none have been shown to be superior to the rest. It is therefore advisable to individualize each case, with the possibility of combining more than one treatment option. Most of these treatments have only shown improvements over the short term. We therefore need to continue searching for therapies that can reduce pain and improve function over the middle and long term - and this is where radiofrequency and the different pain neuromodulation strategies may find an application. Nevertheless, studies of greater methodological quality are needed.



