Introduction
Anterior cruciate ligament (ACL) reconstruction is a widely accepted procedure for the treatment of ACL tears, although it has a 10-20% failure rate at 10 years(1). The results of these revision surgeries are worse than those of primary surgery, with only 27% of patients returning to their previous level of activity(2) and re-rupture rates of up to 12%(1).
There are multiple causes related to the failure of ACL reconstruction, including a new traumatic event, errors in surgical technique, infections, biological failures... and, in up to 4% of cases, alterations in the alignment of the knee(1).
Until a few years ago, osteotomies have been used for the treatment of monocompartmental osteoarthritis associated with varus or valgus alignment of the knee because of their role in load distribution, "relieving" the load on the affected compartment in cases of degenerative disease(3).
Recently, tibial slope has been linked to centre pivot mechanics. Several biomechanical studies on cadaveric specimens have studied the association between sagittal plane deaxations and failure of ACL plasty: Agneskirchner et al.(4) demonstrated in 2004 the relationship between posterior tibial slope values and the tensile forces experienced by both cruciate ligaments, and, in the same year, Giffin et al.(5) showed how decreasing or increasing this slope can improve knee biomechanics and decrease stress on the ACL or posterior cruciate ligament (PCL).
Alignment in the coronal plane also plays a determinant role in the biomechanics of the cruciate ligaments: chronic ACL tears lead to deterioration of the cartilage in the posterior region of the internal tibial plateau, resulting in progressive varus deviation (simple or primary varus) which, over time, will lead to weakening of the lateral ligamentous structures (double varus), characterised by the appearance of a "dynamic varus thrust" under load. In the final stage, the failure of the stabilisers of the posteroexternal corner will result in a triple varus deformity, manifested by a "varus-recurvatum thrust" phenomenon during gait. Several biomechanical studies have shown an increase in the stresses suffered by the ACL(6) in double and triple strains, favouring its rupture (and that of its reconstructions). Won(7) and Noyes(8) demonstrated an increased frequency of varus misalignments in patients requiring ACL revision surgery and Kim et al.(9) demonstrated that inadvertent tibial slope augmentation during proximal tibial valgus osteotomies causes degenerative changes in the ACL.
This is why the paradigm of the role of proximal tibial osteotomy has changed, expanding its range of indications beyond single-compartment osteoarthritis. The 3 objectives of osteotomy in unstable knees are: to prevent progression of osteoarthritis due to joint wear and tear(10), to protect the plasty from overloading the misaligned knee and to restore stability(11).
The aim of this study is to perform a systematic review of the literature on the results of this surgery in patients with previous ACL reconstruction surgery who present instability after surgical stabilisation. For this purpose, we analysed the postoperative results of limb realignment surgery in these indications, referring to stability (objective and subjective), degree of satisfaction, return to daily activities and sports, as well as associated complications.
Methods
This systematic review was conducted in accordance with PRISMA(Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Bibliographic search
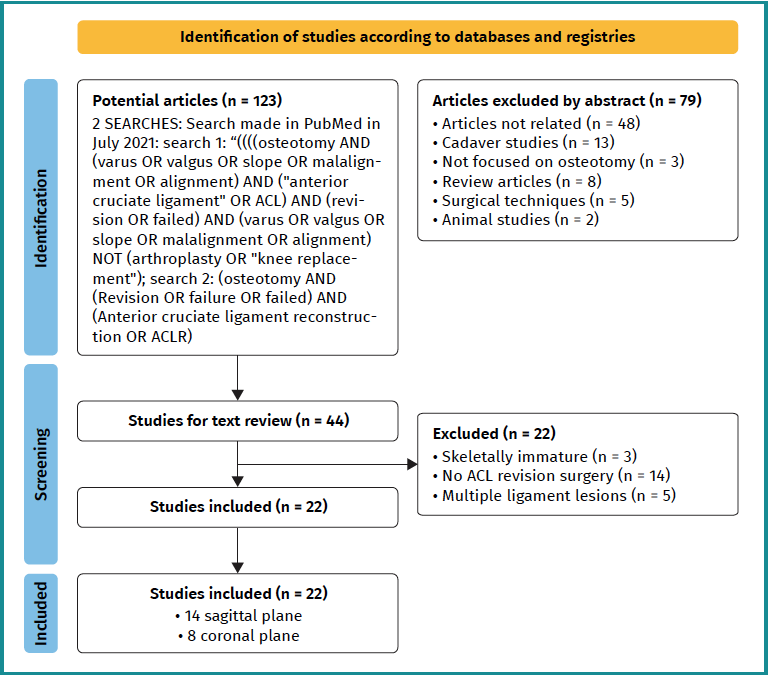
We conducted a systematic electronic database search in Medline, PubMed and Embase in July 2021 to identify clinical studies related to: 1) knee axis alterations as a cause of failure after ACL reconstruction surgery; and 2) the impact of surgical realignment procedures on knee instability after ACL stabilisation surgery. Searches were carried out using the following headings and fields. Search 1: (osteotomy) AND (varus OR valgus OR slope OR malalignment OR alignment) AND ("anterior cruciate ligament" OR ACL) AND (revision OR failed) AND (varus OR valgus OR slope OR malalignment OR alignment) NOT (arthroplasty OR "knee replacement"); search 2: (osteotomy) AND (revision OR failure OR failed) AND (anterior cruciate ligament reconstruction OR ACLR).
Inclusion criteria consisted of: studies focusing on sagittal and coronal plane alterations as a cause of failure after ACL reconstruction surgery and studies including outcomes of ACL reconstruction surgery in conjunction with corrective tibial osteotomies, both with a minimum follow-up of 2 years, skeletally mature patients, English language and human studies. Exclusion criteria included animal studies, basic science studies, cadaveric studies, editorials, reviews, expert opinions, surveys, topical issues and letters to the editor. We also excluded all studies that did not focus on the knee joint. In addition, all references of included studies were reviewed.
Data extraction
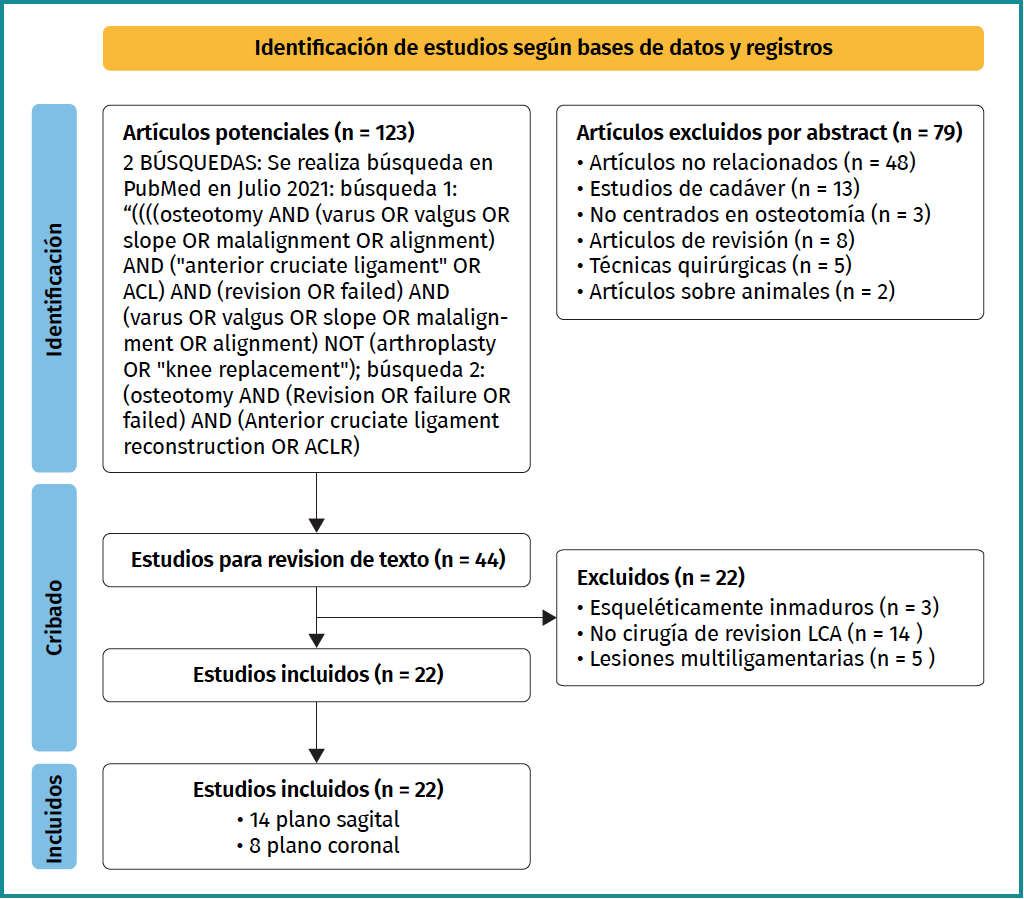
We performed data extraction according to the inclusion and exclusion criteria, as reflected in the PRISMA flow chart (Figure 1). All studies were assessed by two independent investigators (JDR and PC). The summaries of the rest of the studies were read. If there was doubt as to whether the study met the inclusion criteria, the full study was read. The level of evidence of all articles was studied according to Wright's definition(12) published in the Journal of Bone & Joint Surgery. We collected the information obtained from the studies. We assessed pre- and postoperative instability, subjective as well as objective instability sensation with anterior drawer test, Lachman and pivot shift. We measure both coronal and sagittal misalignment, as well as satisfaction and complications. These data were recorded in a Microsoft Excel spreadsheet (Microsoft Corp.).
Bias
In level 3 and 4 studies, it is logical to think that selection biases may exist, due to the lack of randomisation and prospective control groups, especially in populations with heterogeneity of their lesions. We limit this point by ensuring that the authors minimised this bias while admitting the limitations of their study in the publications.
RESULTS
Through manual and electronic reference searching, a total of 123 potentially valid studies were identified. Following the detailed review in Figure 1, we finally included 22 articles, of which 14 dealt with the sagittal profile and 8 with the coronal profile. This gave us a number of 3,925 patients in the sagittal profile group and 563 patients in the coronal profile group. Follow-up of patients ranges from 2 to 23 years. There was heterogeneity in terms of indications, objective and subjective outcomes within the included studies. The most commonly used measurements during patient follow-up were subjective (patient-perceived) and objective (by anterior drawer, Lachman and pivot shift measurement) instability, return to sport and complications. The choice of satisfaction parameters was also varied.
Sagittal profile
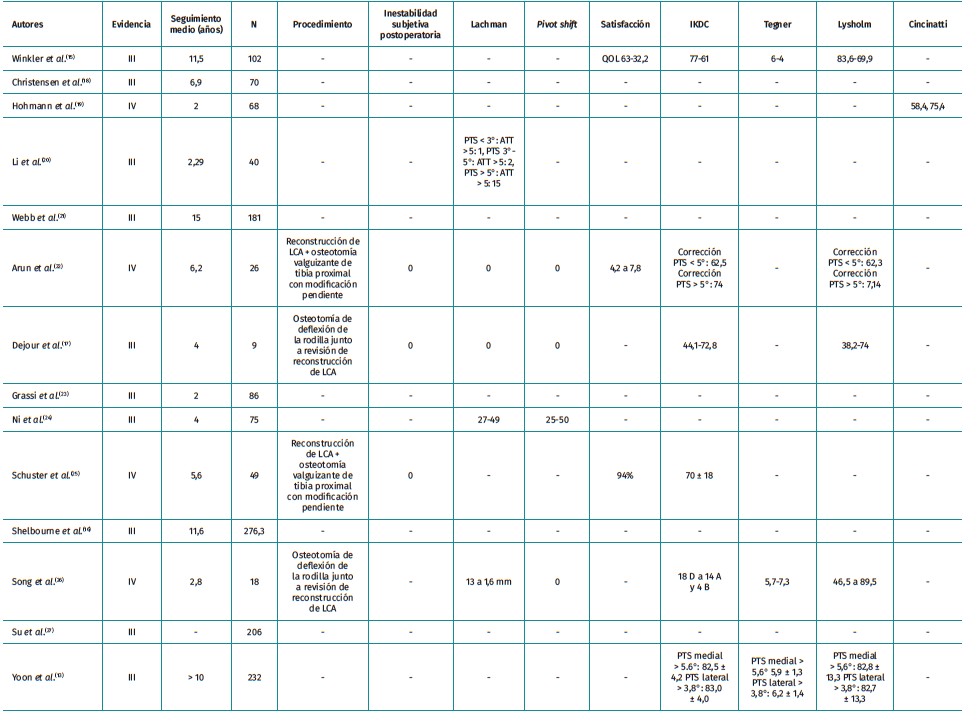
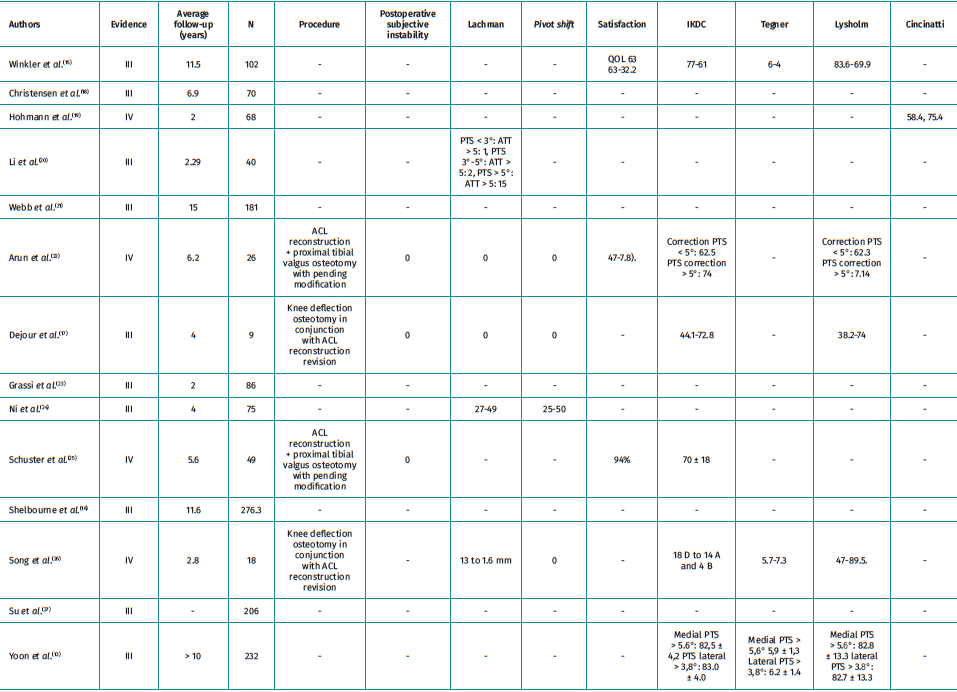
We found 14 articles that met the inclusion criteria. In 11 of them, they recommend knee deflection osteotomy as a treatment for salvage surgery after failed anterior cruciate ligamentoplasty of the knee when there are tibial slope increases. Of these, 3 found no differences in the groups studied. Regarding the limiting value for correction, it seems to be quite widespread that for slopes steeper than 12° , correction may be justified to increase the survival of the plasty. In one study, by Yoon et al.(13), they used Li's criteria arbitrarily as reference values. Regarding the technique of choice for tibial slope measurement, there is considerable heterogeneity in the articles. For most authors, Hudek's method(14), based on magnetic resonance imaging (MRI), is the most accurate, although only 5 of these studies used this form of measurement. Lateral full tibia radiographs were used in 2 studies and lateral short tibia radiographs in 7 studies. As for the results, 8 of the studies do not define the method of measuring the degree of subjective satisfaction, 6 of them use scales such as the International Knee Documentation Committee (IKDC) or the Lysholm scale, and 7 of them do not describe satisfaction measurement scales (Table 1)(13,15-27).
Coronal profile
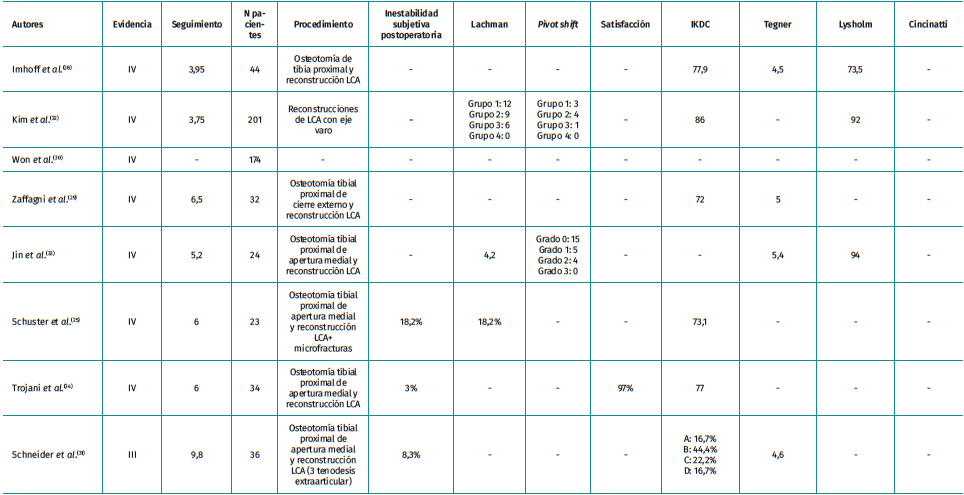
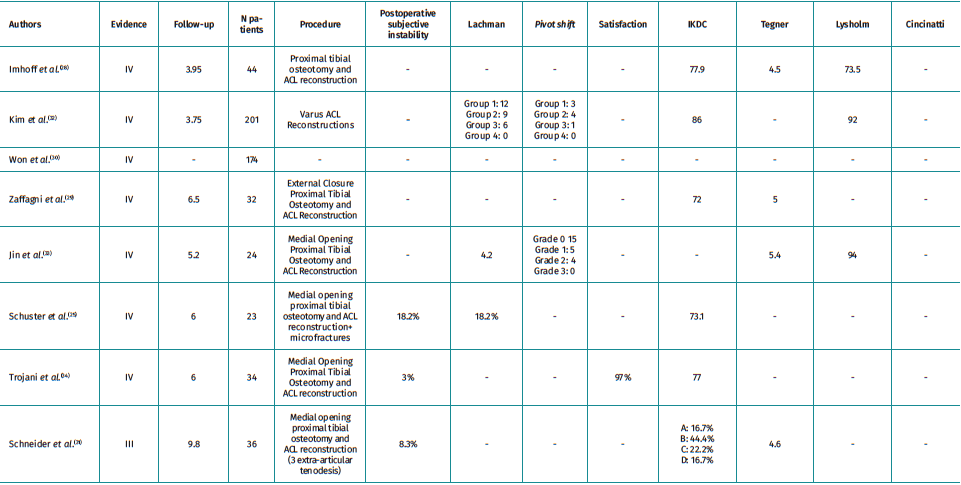
There are 8 articles included in the review (Table 2)(25,28,29,30,31,32,33,34). All but one publication found differences in outcomes after the addition of a tibial osteotomy in revision ACL surgery of varus knees. These studies concluded that varus correction improves the functionality and stability of these knees. As for the measurement technique, in 6 of them it was the mechanical femorotibial angle measured in anteroposterior radiography of the lower limbs under load. One of them used the mechanical axis deviation and one did not define it. None of the articles describe the correction cut-off point.
Satisfaction
All studies used scales such as the IKDC, Lysholm and/or Tegner scales, although in 3 of them objective instability measures were not defined. As limitations, they show series with little follow-up, retrospective and, in half of them, without a control group.
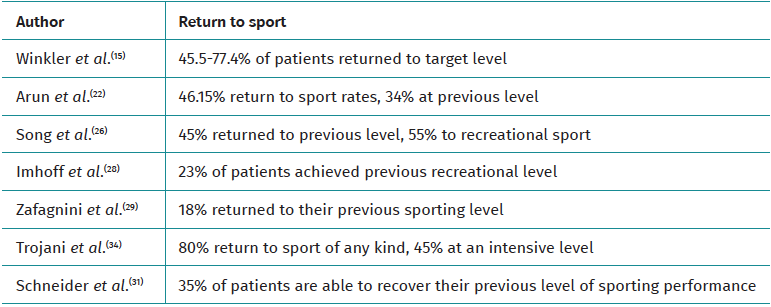
Return to sport
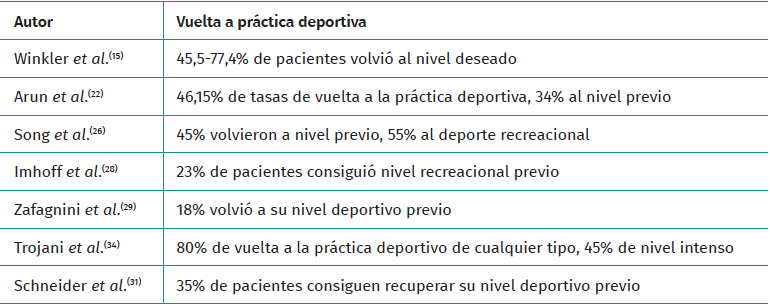
They vary between 18 and 80%, although the definition criteria are heterogeneous and sometimes arbitrary, making comparability very limited (Table 3)(15,22,26,28,29,31,34).
Complications
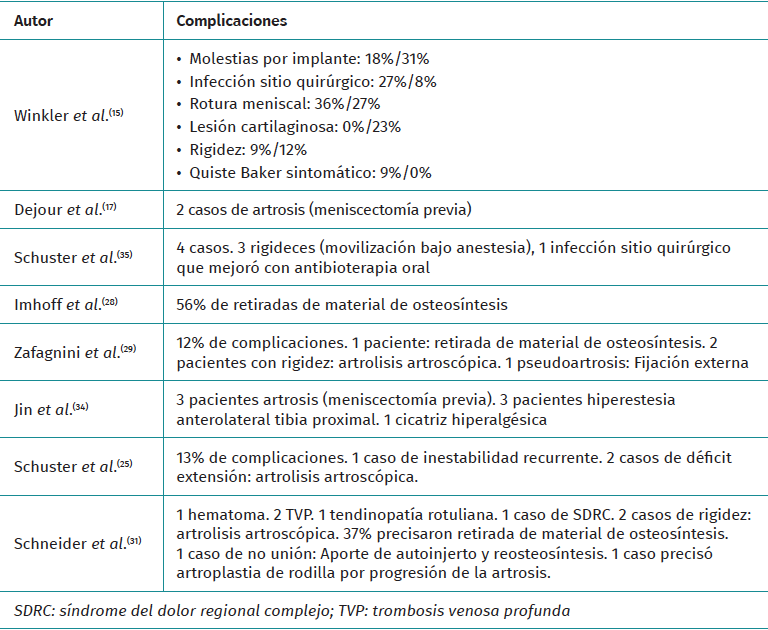
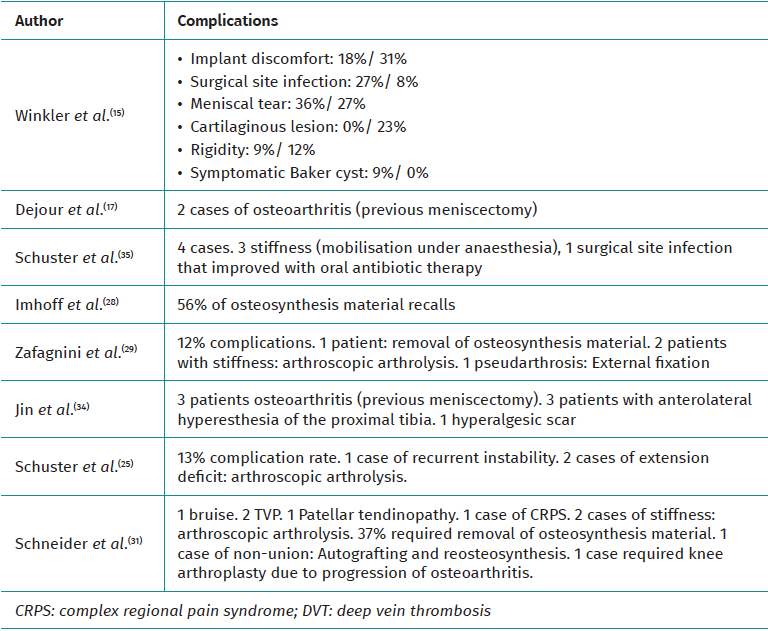
Most of the reviewed studies on coronal profile alterations include a description of the complications, although only 3 of those analysing sagittal profile alterations did so. One study shows a 10% complication rate(15), including stiffness and superficial infections. In another(29), discomfort from osteosynthesis material and superficial infection were the most frequent. In the remaining studies, complications were either not assessed or not specifically described in their text.
Of those who assessed the coronal profile, 5 of them reflect complications. One study(30) shows up to 12% complications (discomfort from osteosynthesis material, stiffness or pseudarthrosis) and another(35) 13% complications, ranging from instability to stiffness. One case of surgical wound hyperesthesia, one case of postoperative pain and one case of persistent varus due to hypocorrection are described. Of note is the article by Schneider(31), where 37% complained of discomfort from the implant and one patient required revision surgery with total knee arthroplasty (Table 4)(15,17,25,28,29,31,34,35).
Discussion
The most important finding of this study is that after ACL plasty rupture and in the presence of a coronal or sagittal axis disturbance, ACL revision surgery together with knee osteotomy improves patients' objective and subjective scales.
The study of axis alterations should be systematically included in the preoperative imaging protocol. In the event that this alteration is confirmed and in line with the findings obtained from this systematic review, limb realignment surgery should be considered and performed either in isolation or in combination with ACL revision surgery(14).
This can be performed alone, as an associated gesture or in 2 stages, preceded by ACL salvage surgery in cases of persistent instability. On this last point, there are contradictory results. In the Shelbourne study(16), despite acknowledging that increased slope is associated with an increased risk of ACL plasty rupture, they do not recommend prophylactic corrective osteotomy or primary surgery, as the risk of rupture of the contralateral ACL or revision plasty is low. In addition, the complication rate is not negligible, with a 13% complication rate (although generally minor); and up to 56% of patients will receive a second surgery for removal of the osteosynthesis material, due to discomfort with it.
In Winkler's study(15), it can be seen how patients with tibial slope above12° have higher failures and worse results in objective and subjective tests, recommending realignment surgery to improve these assessment parameters. Dejour et al.(17) evaluated the results of ACL revision surgery in conjunction with knee deflection osteotomy, with a minimum follow-up of 2 years, concluding that this tibial slope correction surgery protects the plasty from biomechanical overloads. Giffin et al.(5), in a biomechanical study, demonstrate that an increase in this slope leads to an anterior tibial translation at rest, which increases with load. Their findings suggest that decreasing this slope may have a protective effect in the ACL-deficient knee. Furthermore, just as decreasing the tibial slope has a protective effect on the ACL, the same effect on the PCL can be expected if the posterior tibial slope is increased. This may be an alternative for older patients with degenerative changes in whom ACL reconstructive surgery is a relative contraindication.
With regard to the coronal plane, Zaffagnini et al.(17) combine ACL revision surgery with proximal tibial valgus osteotomy, obtaining improvements in functional, stability and alignment results, although they concluded that once monocompartmental osteoarthritis was established, the realignment osteotomy did not prevent the progression of these degenerative changes in the medial compartment. Even so, they improve all parameters and achieve a return to sport of 20%.
It is evident that, despite complications, realignment surgery in conjunction with ACL revision improves functional outcomes and has good rates of return to sport, reaching rates of 18-80%(15,22,26,28,29,31,34), as can be seen in this systematic review. Studies evaluating the combination of ACL revision surgery and anterior tibial osteotomy tended to report higher postoperative activity levels compared to osteotomy alone. However, postoperative activity scores on the Tegner scale improved in all groups of patients, even those with ACL insufficiency who were treated by osteotomy alone. This highlights the importance of correct alignment for the performance of activities of daily living, as misalignments can lead to pain both from overloading one of the compartments and from ligamentous stress and the associated feeling of instability, which adds to the incompetence of the ACL. This review concludes that there is an increased likelihood of failure of ACL reconstruction surgery in the presence of misalignments in the coronal and/or sagittal planes of the knee. Furthermore, current literature suggests that, in these cases, the addition of a corrective tibial osteotomy may reduce this risk. However, there is currently a lack of comparative studies between isolated ACL reconstruction surgery and combined surgery with tibial osteotomy, which are essential for a complete assessment of the risk-benefit profile of both options.
There are several limitations to this study. First, this systematic review almost exclusively includes studies with levels 3 and 4 evidence (prospective and retrospective series). Second, many of the studies evaluated are more than 10 years old. In addition, data collection and outcome assessment parameters were quite heterogeneous, making it difficult to infer results. Third, a large number of the studies had selection biases due to their non-randomised design and lack of a prospective control group.
Conclusions
Proximal tibial osteotomy is an effective treatment in the management of knees with anterior instability associated with coronal and sagittal plane disturbances.