Introduction
The concept of anterior ankle impingement (AAI) has undergone significant changes in recent decades. In the last decade, ankle arthroscopy has developed considerably and is establishing itself as a standard in the diagnosis and treatment of different foot and ankle disorders(1,2). Until a few years ago, ankle arthroscopy was mainly indicated for talar osteochondral injuries or anterior impingements, usually as sequelae to sprains; however, its indications have now been greatly expanded(3). In the case of AAI, many studies have reported good results after simple resection of the interposed soft tissue or osteophytes, though with the recurrence of symptoms after some time(4). There is now ample scientific evidence to support the association between many of these impingements and ankle instability, which implies the need to combine resection with ligament repair or reconstruction techniques(3,5,6,7).
The question that arises is whether the concept of AAI, specifically referred to those cases caused by soft tissue, is still relevant today or whether these are simply associated lesions secondary to an underlying disorder related to chronic instability. The present article analyzes the current status of AAI and its relationship to chronic ankle instability, and discusses whether it can still be considered an isolated disease condition.
Definition
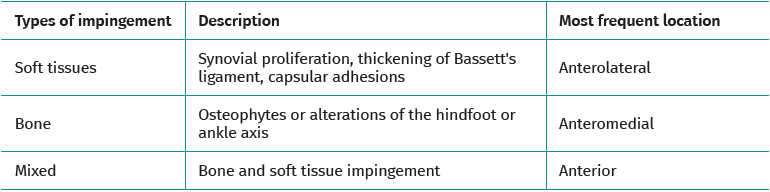
Anterior ankle impingement is defined as pain and/or limitation of range of motion that occurs with dorsiflexion of the ankle, due to the presence of soft tissue or bone interposed between the joint surfaces. A distinction is made between soft tissue impingement (synovial proliferation, thickening of Bassett's ligament, capsular adhesions), bony impingement (osteophytes or alterations in the ankle or hindfoot axis) (Figure 1) and mixed impingement (Table 1). AAI in turn can be subdivided into central, anterolateral and anteromedial impingement(8), with the first two being the most common presentations(9). Anterolateral AAI usually involves soft tissue, while anteromedial AAI is usually caused by a spatial conflict between osteophytes of the talar neck and anterior to the medial malleolus in dorsiflexion(9,10). AAI is the most common cause of anterior ankle pain that worsens with dorsiflexion. However, posterior impingement may be more frequent in certain patient groups, such as dancers or football players, due to repetitive movements in forced plantar flexion(4).
Morris first described AAI in 1943(11). Years later, McMurray coined the term "footballer's ankle" (12). In 1957, O'Donoghue referred to "impingement exostoses" (13). Wollin, in 1950, first described soft tissue impingement involving Bassett's ligament(14,15). In 1991, Ferkel and Scranton described the pathophysiology of anterolateral ankle impingement syndrome, indicating that an ankle sprain that injures the anterior talofibular ligament (ATFL) may result in incomplete healing of the latter(15). Repetitive movements can cause synovitis and fibrosis, forming a painful mass of soft tissue in the joint space. The pain should disappear weeks after complete healing of the ATFL.
Etiopathogenesis
Anterior ankle impingement was originally described as a bony impingement caused by exostoses or osteophytes, without considering etiologies other than primary osteoarthritis or repetitive trauma to the ankle. Subsequently, the concept of soft tissue AAI was introduced, based on observation of the proliferation of anterolateral scar tissue following an ankle sprain. AAI can be post-traumatic (ankle fractures, sprains), post-surgical (scar tissue) or due to sports microtrauma. In soft tissue impingement, meniscoid lesions, scar tissue hypertrophy and Bassett's ligament impingement have been described as the cause of pain(16). The presence of osteophytes or scar tissue is not necessary for AAI to occur; a displaced calcaneal fracture subjected to orthopedic treatment can cause horizontalization of the talus and anterior impingement(17). In the sequelae of distal tibial fractures or physeal growth disturbances, a recurvatum deformity may be the cause of pain, due to anterior impingement of the ankle(18). Osteoarthritis of the ankle is characterized by the presence of osteophytes in its early stages, which may lead to AAI(19). Chronic ankle instability and post-traumatic injuries following fracture are the most common causes of such osteoarthritis(20).
Kissing osteophytes, which refer to the simultaneous presence of osteophytes on the anterior border of the talus and tibia,have been considered a source of anterior ankle pain due to the mechanical impingement they cause upon impact with each other during movement(21). However, this theory has now been abandoned, as many authors have shown that there is no real contact between the two osteophytes during ankle dorsiflexion(22). The tibial osteophyte is more medial and the talar osteophyte is located more lateral. Other studies have shown that osteophytes are asymptomatic in 45% of football players and in 59% of dancers(23).
The association between AAI and chronic ankle instability is a more recent concept(5,24,25). Ferkel considered that the presence of anterolateral ankle impingement (ALAI), although related to inversion trauma, excludes the diagnosis of ankle instability(10). However, different studies reported recurrence of the symptoms after the isolated treatment of anterolateral impingement through simple resection of the osteophytes or interposed soft tissue, such as a persistent sensation of instability or new sprain episodes, as described by Katakura et al.(26) in a systematic review on ALAI and its relation to ankle instability. They identified 8 studies with level IV evidence, of which 5 mentioned the presence of recurrent instability or sprains. One study described the presence of concomitant ATFL lesions. The ankle sprain recurrence rate after simple impingement resection treatment ranged from 8-20%. The authors concluded that simple resection of hypertrophic tissue in ALAI has a limited level of scientific evidence, and suggested that all patients to be surgically treated for AAI should also be checked for ATFL status.
Vega et al. reported that the inferior fascicle of the ATFL is located extra-articular, while the superior fascicle is intra-articular, which may imply a reduced healing potential, as seen with the anterior cruciate ligament(27). Lack of adequate healing of the superior fascicle of the ATFL can lead to micro-instability(5,28,29), a concept previously described in the shoulder(30). In the past, many of these patients were diagnosed with functional instability, a concept coined by Freeman in 1965(31). Radiological stress tests have significant limitations in terms of sensitivity(32) and great variability in the range of physiological values and reproducibility(33,34). As a result, they are not considered necessary for the diagnosis of acute or chronic ankle instability(35), since they may underdiagnose more subtle instabilities. The concept of micro-instability has represented a paradigm shift in the assessment and management of these patients who previously would have been diagnosed and treated as cases of ALAI. This has led to a therapeutic approach focused on joint stabilization, leaving the treatment of impingement (whether of bony or soft tissue origin) as a matter of secondary relevance.
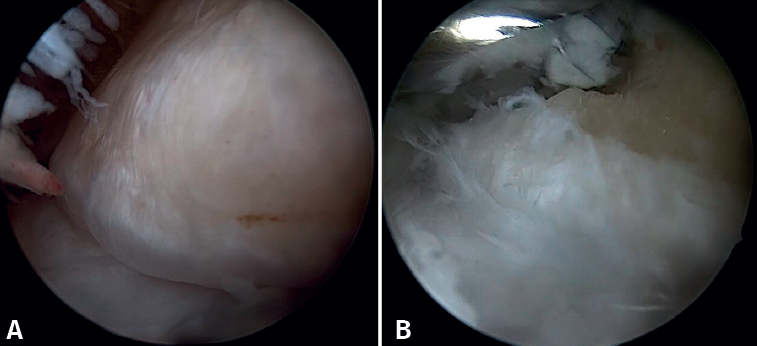
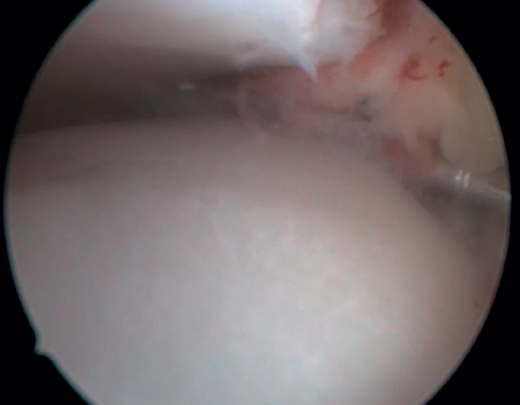
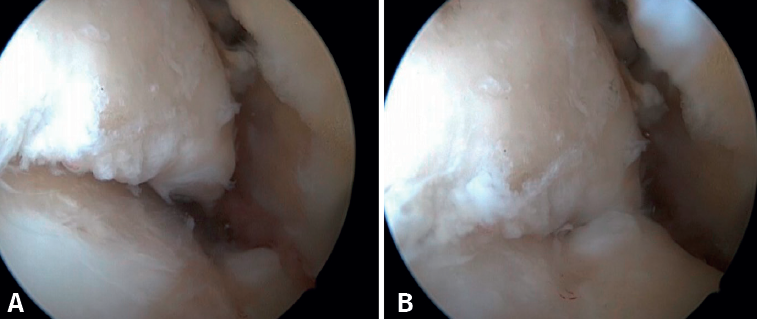
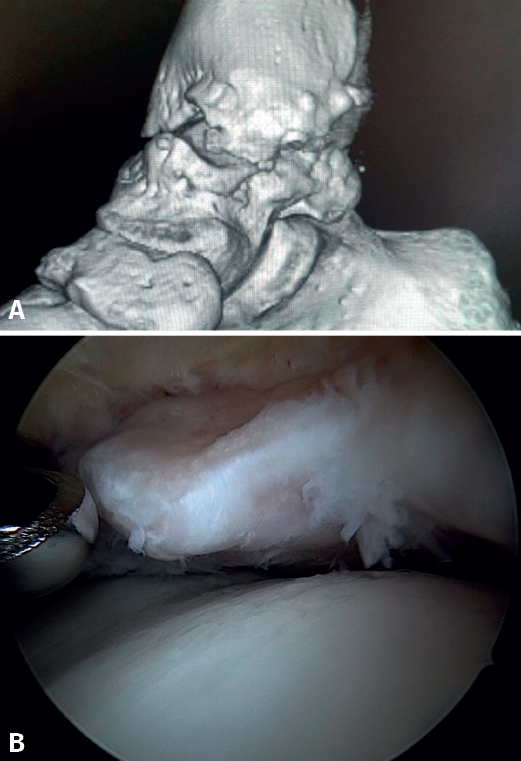
Bony AAI due to osteophytes has also been linked to the presence of chronic instability. It has been postulated that altered joint kinematics secondary to ligament insufficiency favors the development of osteophytes in the anterior region of the tibia and talus(36,37). Recent studies have questioned the theory of repeated capsular traction as the origin of osteophytes in sports(38), as it is easily demonstrated that osteophytes are located intra-articular within the capsular insertion, in the context of ankle arthroscopy (Figure 2). Therefore, ankle dorsiflexion arthroscopy is essential to safely resect osteophytes without damage to the capsule or overlying structures, whereas the classical traction technique (invasive or otherwise) would make resection extremely difficult, and is thus not recommended nowadays for routine use(3,39). Vega distinguished between two types of osteophytes(3), according to whether they are caused by repetitive trauma (peak-shaped) or instability (visor-shaped). The concept of micro-instability is associated with repetitive micro-trauma, which could be the origin of osteophytes with this characteristic morphology (Figure 3).
Another concept is that of rotational instability, in which the anterior part of the deltoid ligament suffers degenerative injury due to the micro-movements in anterior drawer and internal rotation caused by primary anterolateral instability. Up to 40% of all chronic instabilities are considered to be of this type(3). Medial and lateral pain may be the only clinical manifestation, in the same way as AAI.
Bassett's ligament has long been considered a pathological structure and a cause of anterolateral impingement, so resection of this ligament was included in the surgical protocol for the treatment of AAI(40). This ligament is the intra-articular portion of the anteroinferior tibiofibular ligament of the syndesmosis. In relation to its involvement in AAI, it seems to play more of a victim's role, since the micro-movements of the talus in the mortise produce micro-traumatisms that can thicken or damage the ligament. Nowadays, this ligament is considered to have proprioceptive capacity, due to contact with the talar dome at ankle dorsiflexion; it is therefore advised to avoid its resection(41).
Clinical manifestations
The pain generally appears during movement and subsides or disappears at rest, i.e., it has clear characteristics of mechanical pain. It is usually located on the anterior aspect of the tibioperoneal-talar mortise, either along its entire length or locally on the medial or lateral groove. The pain may be associated with the presence of edema and limitation of ankle dorsiflexion. In anterolateral ankle impingement, the persistence of any of these symptoms for more than 6 months after an ankle sprain is considered a clinical diagnostic criterion. These symptoms are often associated with recurrent sprains or subjective feelings of instability or kinesiophobia. The patient usually recalls having suffered a sprain, which makes us suspect a strong causal relationship between the presence of AAI and chronic ankle instability. Patients often report limitations associated with pain, stiffness, locking and/or clicking when climbing stairs or slopes and, in general, any activity requiring forced dorsiflexion of the ankle. Clinically, the signs and symptoms of AAI overlap with those of chronic ankle instability, which may be taken as a further confirmation of their close relationship.
Physical examination
The Molloy test(42)has been described for the exploratory diagnosis of AAI; it is performed by anterolateral painful palpation of the anterior region of the ankle, with increased pain being noted on dorsiflexion of the ankle. A sensitivity of 88% and a specificity of 94.8% has been reported(42). The presence of pain on palpation at the talar insertion or on the anterior aspect of the external malleolus, or the presence of an anterior ankle drawer would suggest possible ankle instability associated with ATFL injury; in our experience, this happens often. Liu(43) considered pain with single-leg squat and pain with ankle dorsiflexion to be diagnostic criteria for ALAI.
Palpation should be used to locate the pain in the anterior mortise at the joint line and at the grooves. Pain in the anterior aspect of the external malleolus may be related to ATFL injury, and we should avoid confusion with neighbouring regions such as the sinus tarsi (which may indicate the presence of subtalar arthrosis, subtalar instability, valgus foot impingement, etc.), peroneal tip pain (due to peroneal subfibular impingement), pain in the syndesmosis due to instability at this level, lateral talar osteochondral lesions, etc.
AAI, especially bony AAI, may result in a loss of the last degrees of ankle dorsiflexion, which may be evidenced on examination. The Lunge test is performed by comparing the distance from the toe of the healthy foot to the wall, achieving contact of the patella with the same wall without lifting the heel off the ground, with the shorter distance of the ankle with limitation of dorsiflexion. The test is able to override the action of the calf, but not the presence of equinus due to other causes, such as a shortened soleus or shortening of the posterior capsule; it is of little use in differentiating these causes from bony anterior block. The same applies to hyperpronation of the foot, which can compensate for this dorsiflexion defect. Nevertheless, it is a useful test, provided that these differential diagnoses can be ruled out. The Silfverskiöld test also allows us to assess whether the loss of dorsiflexion is, in fact, a case of calf-dependent equinus.
In all patients it is important to detect the presence of infra- or supra-malleolar varus or valgus axial deviations that can lead to osteoarthritis with the consequent formation of osteophytes; to this end, it is essential to examine these patients in the standing position.
Imaging diagnosis
Ankle and foot weight-bearing radiography is used to detect alterations in mechanical alignment of the ankle. Osteophytes may be clearly visible on lateral ankle radiographs, although Van Dijk et al.(8) described a radiological projection to detect more lateral locations, involving a lateral projection with 30° of external rotation. This projection doubles the sensitivity and specificity of plain lateral radiography(44). Computed tomography (CT) is the definitive test to locate and visualise the osteophyte in three dimensions.
In case of suspected soft tissue AAI, magnetic resonance imaging (MRI) is considered the technique of choice, although some authors consider physical examination to be more sensitive(45). MRI arthrography increases the ability to detect AAI with a sensitivity of 96% and a specificity of 97%(46).
Arthroscopic diagnosis
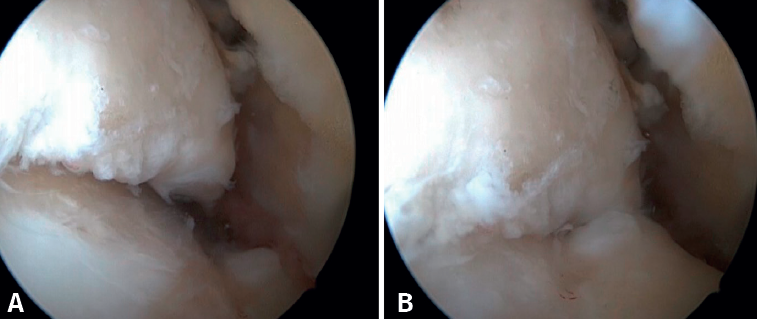
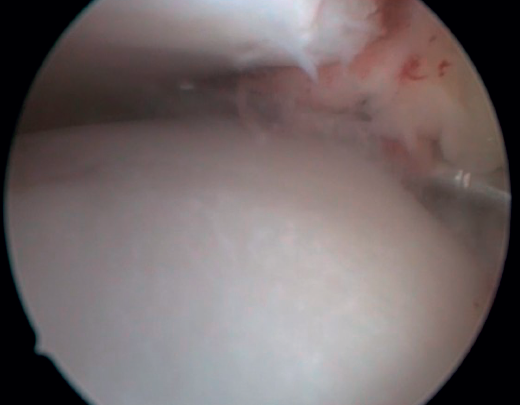
The confirmation of AAI is made by direct vision during arthroscopic examination (Figure 4). This technique allows us to visualise the entire joint, assess the state of the articular cartilage and ligaments, detect the presence of capsular adhesions, synovitis, synovial thickening, loose bodies, etc. It also allows us to carry out functional tests to reveal possible associated instabilities or to assess how the soft tissues causing pain suffer impingement. In our experience, the presence of ATFL lesions is very frequent.
Conservative management
Conservative management varies depending on the disorder associated with AAI. In cases of altered hindfoot alignment, corrective insoles may be useful. For the associated chronic instability, the patient may find relief of symptoms with the use of ankle braces or functional bandages. Heel cups or raised heel shoes can reduce impingement and the intensity of pain.
Intra-articular infiltrations of corticosteroids with local anesthetic, hyaluronic acid, platelet-rich plasma, etc. may have some effect in terms of temporary pain control(47).
Surgical treatment
Arthroscopy has become the gold standard in the treatment of AAI and its associated causes. This technique allows precise diagnosis and visualization of the type of impingement in a dynamic manner, by applying the pertinent maneuvers. Even in cases of large osteophyte formations, arthroscopy is feasible using the forced dorsiflexion technique, since the insertion of the joint capsule into the tibia is located a few millimeters dorsal to them. Traction is not necessary and may even be considered contraindicated in this disease condition, due to the risk of tendon or neurovascular injury.
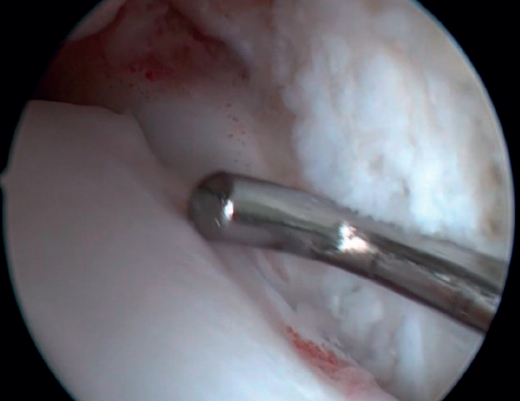
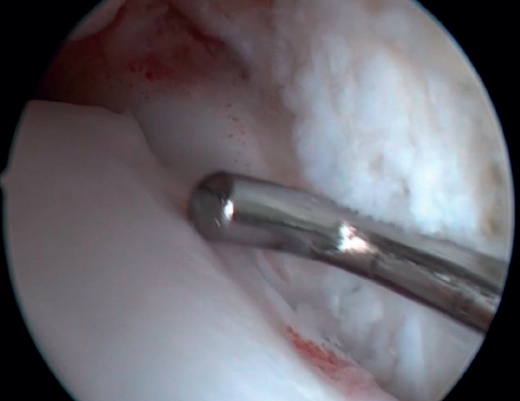
Resection of the osteophyte is performed by displacing from the top, and gradually reducing it until the joint zone is reached (Figure 2). A basket forceps can be used to resect the area closest to the joint (Figure 5). It is often useful to exchange the viewing and working portals in order to visualize and completely resect the osteophytes. In the case of soft tissue impingement, a 3.8 or 4 mm synoviotome is usually sufficient. The vaporizer is useful in the case of compact impingements, typical of post-traumatic conditions or re-interventions, and also for delimiting the bony part of the osteophyte before resection.

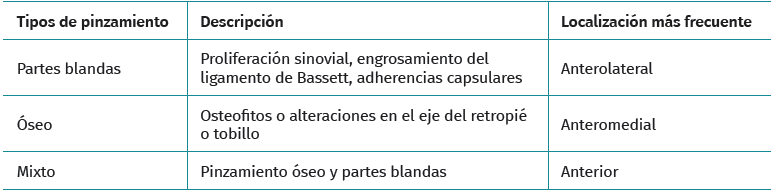
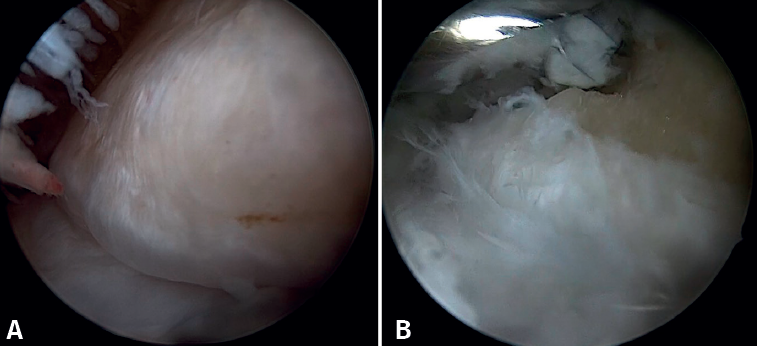
Bassett's ligament should be preserved as long as it does not have a pathological appearance, ruling out thickening, partial tears or reciprocal lesions on the anterolateral surface of the talus (Figure 6), which are associated with anterolateral or rotational instabilities. The peroneal insertion is used as a reference to locate the distal insertion of the ATFL. The deltoid ligament at the medial groove should be inspected if associated rotational instability is suspected. During arthroscopy, direct ligament repair can be performed using sutures and anchors.
Conclusions
In summary, the approach to AAI has evolved significantly: once considered to be an isolated disorder, it is now regarded as a complex syndrome often associated with ankle instability. This paradigm shift has been made possible thanks to advances in arthroscopy and the development of new concepts such as micro-instability. Arthroscopy not only allows a more accurate diagnosis, but also facilitates treatment of the different affected structures. In this way, it is possible to reduce the likelihood of symptoms recurrence compared with the situation observed when impingements were treated on an isolated basis. In order to more precisely establish the relationship between instability and anterior ankle impingement, it is essential to conduct and design new studies capable of providing more robust data and of further improving the management of this disorder.