Introduction
Injuries affecting the syndesmosis (the fibrous attachment between the tibia and fibula at the ankle) and the medial ligament complex (deltoid ligament) are of great importance in the overall stability of the tibiotalar joint(1). Because they are not as common as lateral sprains, they sometimes go unnoticed or are underdiagnosed, leading to chronic instability, persistent pain and, in the long term, early osteoarthritis(2).
The syndesmosis is composed of the anterior tibiofibular ligament, the posterior tibiofibular ligament, the interosseous ligament and the transverse ligament(3). Each of these elements is involved in containing the joint against axial and rotational loads. The medial complex, consisting of the superficial and deep deltoid ligament, ensures stability in the frontal plane and prevents excessive eversion(4).
The arthroscopic approach has established itself as a highly valuable diagnostic and therapeutic tool. On the one hand, ankle arthroscopy offers a more accurate diagnosis by allowing direct observation of ligament integrity, the presence of chronic synovitis, and associated osteochondral lesions(5). On the other hand, it facilitates minimally invasive surgical procedures, with less morbidity than open approaches, and with potentially shorter recovery times.
This chapter reviews the anatomical and biomechanical aspects of the syndesmosis and medial ligament complex, the relevance of their injuries, the use of arthroscopy in their diagnosis and treatment, and the surgical techniques most endorsed by the current literature.
Anatomy and biomechanics
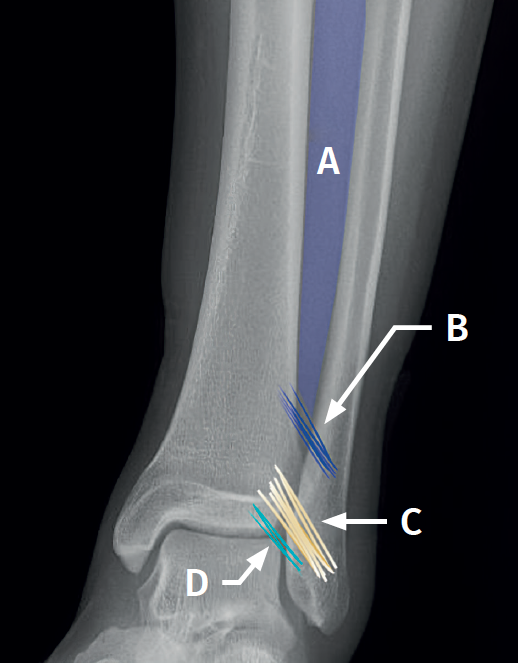
Syndesmosis (Figure 1)
The syndesmosis is a fibrous ring that joins the tibia and fibula distally(1). Its main function is to maintain the congruence of the tibiofibular mortise and to allow physiological micromovements of separation and rotation of the fibula with respect to the tibia(6).
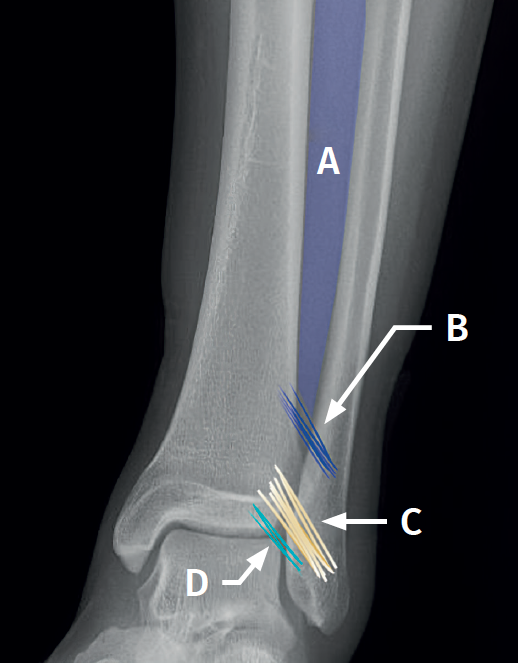
It is composed of:
- The anterior tibiofibular ligament (ATFL). Considered to be the first to be injured by external rotation or forced dorsiflexion forces. It extends obliquely from the anterior tubercle of the distal tibia, approximately 5 mm above the joint surface, to the anterior tubercle of the distal fibula, running proximal-medial to distal-lateral and crossing the anterolateral corner of the talus(7).
- The ATFL has a constant distal fascicle (ATFL-DF) that contacts the anterolateral corner of the talus when the ankle is in neutral position. The distal fibers of the ATFL-DF continue with the upper bundle of the anterior talofibular ligament(8).
- The posterior tibiofibular ligament (PTFL), which is stronger than the anterior ligament. It extends from the posterior tibial malleolus to the posterior tubercle of the fibula and runs proximal-medial to distal-lateral. It forms an angle of 20º to40° with the horizontal plane.
- The interosseous ligament (IL), a distal thickening of the interosseous membrane that acts as a "spring" or dynamic stabilizer.
- The transverse ligament, located in the most posterior part, and considered by some authors as the distal portion of the PTFL.
Arthroscopic anatomy of the syndesmosis
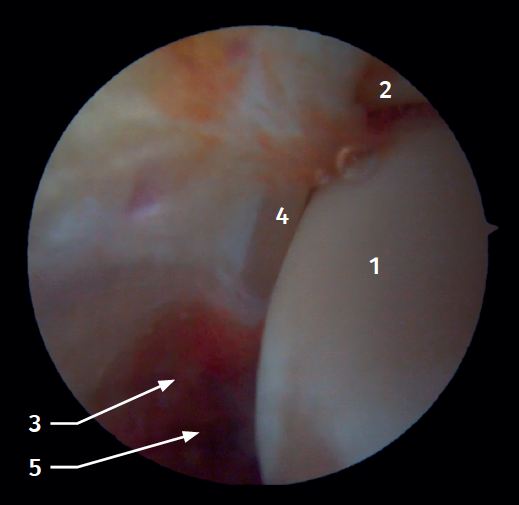
Anterior arthroscopic view
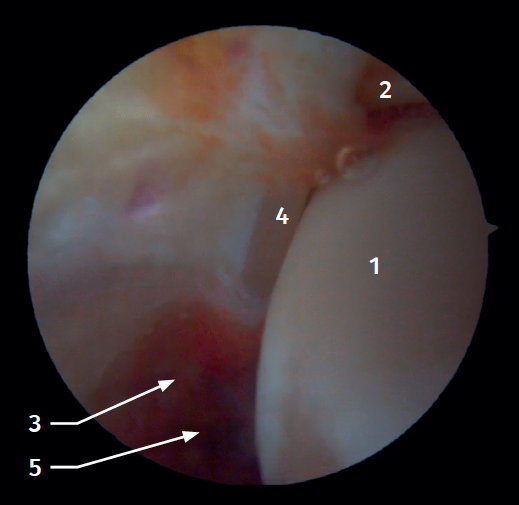
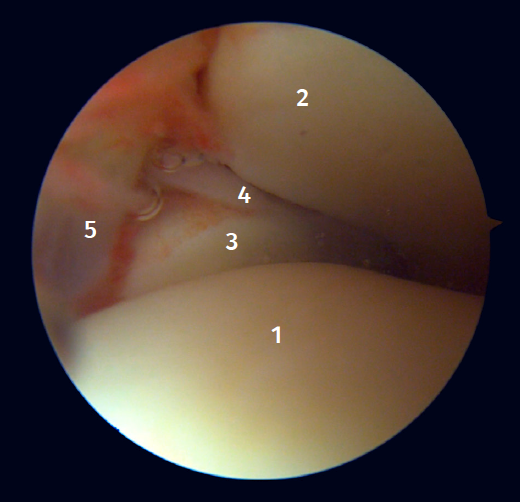
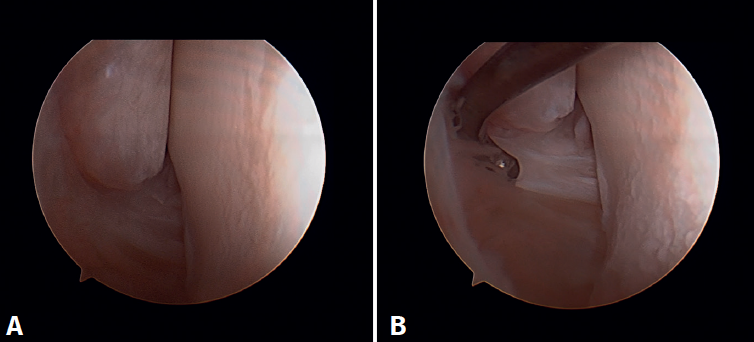
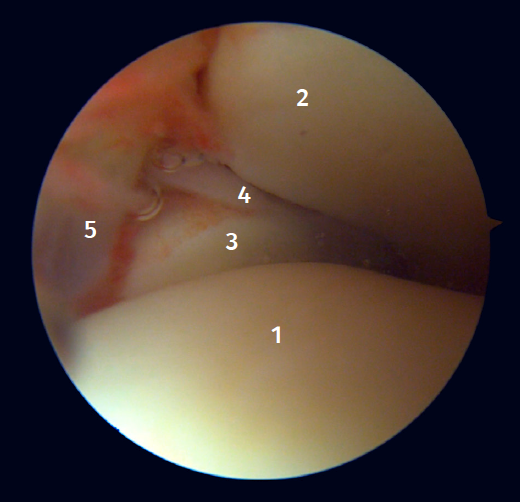
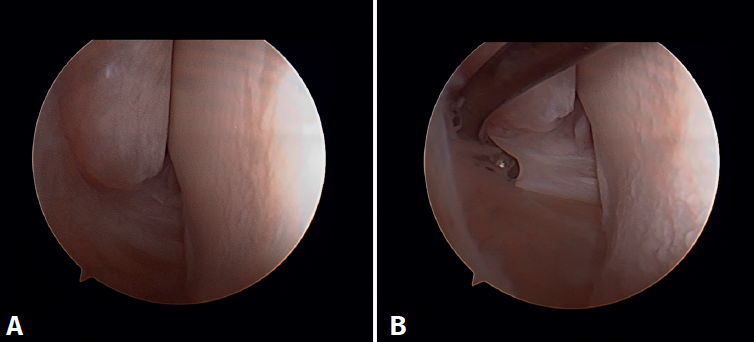
Twenty percent of the ATFL is intra-articular(7). On adopting an anteromedial access of the ankle, directing the arthroscope laterally, we can see the distal fibers of the ATFL with their oblique distribution and their continuation with the anterior talofibular ligament (Figure 2). If we move into the tibiotalar joint, we see the distal tibiofibular joint with the syndesmotic recess occupied by synovial tissue (Figure 3).
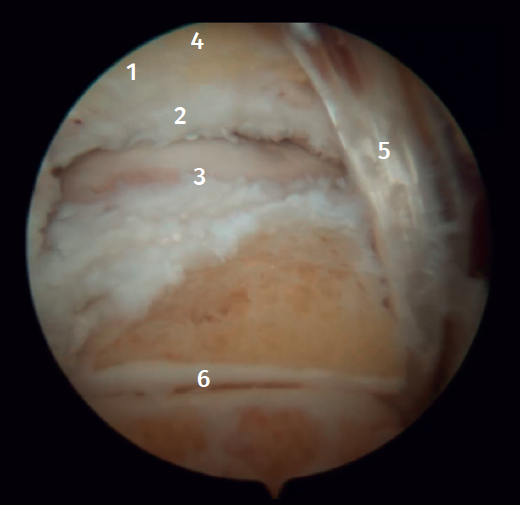
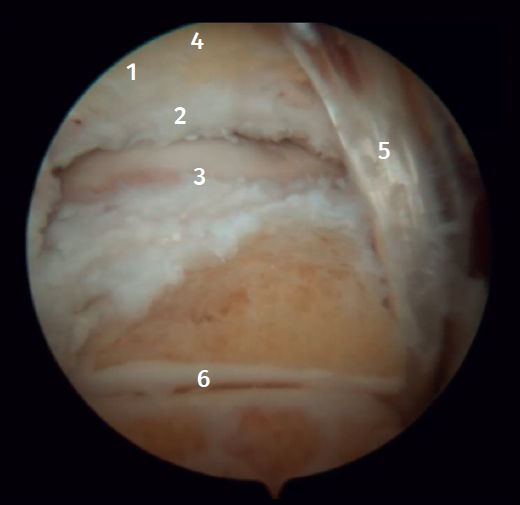
Posterior arthroscopic view
From the posterolateral approach we identify the lateral (fibular) malleolus and, from here, we visualize the intra-articular fibers of the PTFL, which run obliquely and insert into the distal portion of the tibia. We also see the distal thickening of the PTFL (transverse ligament) in continuity with the posterior lip of the distal tibia (Figure 4).
Medial complex
The medial ankle complex, also known as the medial collateral ligament, is a broad, tough fibrous structure located on the medial (internal) side of the joint. Anatomically, this ligament exhibits a fan- or delta-shaped configuration and is made up of two main layers: superficial and deep(9).
The superficial layer is composed of several bands which are divided into:
- The tibionavicular ligament, which arises from the anterior aspect of the medial malleolus and runs towards the navicular bone.
- The tibiocalcaneal ligament, with insertion in the sustentaculum tali.
- The tibiospring ligament, which reinforces the junction with the spring ligament (calcaneonavicular ligament) and stabilizes the medial aspect of the ankle.
- The superficial tibiotalar band, which is directed towards the medial aspect of the talus, reinforcing containment.
The deep layer in turn is composed of:
- The deep anterior tibiotalar ligament, which arises from the anterior aspect of the medial malleolus and inserts on the medial surface of the talus.
- The more robust deep posterior tibiotalar ligament, which runs to the posterior portion of the talus and contributes to anteroposterior stability.
Both layers are in close relationship with the tibialis posterior tendon sheath, which enhances mechanical effectiveness in containing the joint, counteracting excessive hindfoot eversion and avoiding lateral translation of the talus.
Arthroscopic anatomy of the medial complex
Arthroscopy allows us to see the deep fibers of the deltoid ligament, corresponding to the intra-articular portion of the ligament. Medial and proximal to the tip of the malleolus we have the insertion of the deep layer of the deltoid ligament. If there is no injury, we will see the anterior portion of the deep tibiotalar fibers. When injury is present, we can visualize the intermediate and posterior portion. The superficial bands, due to their more external location, are not visible by arthroscopy, unless there is no lesion of the deep bands (Figure 5).
Biomechanics
The deltoid ligament and syndesmosis act together to limit movement of the fibula relative to the tibia, mainly blocking external rotation of the talus. This effect is achieved by keeping the mortise reduced, avoiding lateral displacement of the talus towards the lateral malleolus.
In practice, the deltoid ligament and the syndesmosis should be considered as a single unit performing the same biomechanical function. Therefore, when a lesion of one of these structures is detected, it is essential to examine the other, since the lesions are very often combined(10).
Epidemiology and clinical relevance
Although isolated lesions of the syndesmosis or medial complex represent a smaller percentage than lateral lesions, their relevance has been increasing. Epidemiological studies in contact sports athletes (football, rugby, basketball) describe that 10-20% of all ankle sprains may involve some degree of syndesmotic injury(11). These injuries can be associated with significant morbidity and a delayed return to sports compared to an isolated lateral ankle sprain(12).
The posterior syndesmosis plays the most important role, providing 40-45% of the resistance to diastasis, while the ATFL contributes about 35%. Injuries to two of the components of the syndesmosis result in a loss of more than 50% of diastasis resistance, which can lead to instability(13).
Isolated deltoid ligament injuries account for approximately 3-4% of all ankle ligament injuries(14). Isolated injury to the deltoid ligament usually affects the superficial portion, is rotationally stable, and has a good prognosis. In contrast, in deltoid injuries associated with injury to the syndesmosis, rupture is complete in both layers (deep and superficial)(15).
Diagnosis
A correct diagnosis is essential, as many injuries are underdiagnosed and will lead to sequelae. The most important point is to be able to differentiate between stable injuries, which can be treated on a conservative basis, and unstable injuries.
Clinical assessment
Patients often present with anterior ankle pain, a feeling of instability and limited dorsiflexion. Specific clinical tests include:
- Squeeze test. This test is more specific of syndesmosis injuries. With the patient seated, the examiner presses with both hands on the tibia and fibula, starting just above the ankle. If the pressure causes pain in the distal syndesmosis, injury to its ligaments is suspected.
- The dorsiflexion maneuver. This is performed to push the wider anterior portion of the talar trochlea into the ankle mortise, causing separation of the distal fibula and tibia and pain in the distal tibiofibular syndesmosis.
- Deltoid stress maneuver. This is performed with the patient seated on the stretcher and the feet dangling. First, valgus pressure to the heel is applied, comparing the response with that of the sound ankle. The anterior drawer maneuver is then performed and the result is also contrasted with that of the contralateral side. The external lateral ligament is also involved in anterior drawer stability.
- Selective palpation of the syndesmosis and deltoid ligament. Pain on deltoid palpation is associated with injury, with Hinterman reporting a correlation of 100%(16). In contrast, for the diagnosis of syndesmotic injuries, the figure drops to 56%(17).
Imaging tests
- Plain radiography: in anteroposterior, mortise and lateral views, signs of diastasis of the syndesmosis are observed if the tibiofibular space exceeds 5-6 mm or in the absence of tibiofibular overlap below 6 mm. In many cases the degree of diastasis is not clearly visible in subacute or chronic stages.
- Computed tomography (CT): this technique helps to assess the position of the fibula in the tibial incisura and to detect small anterior or posterior subluxations.
- CT in weight bearing: most useful in cases of suspected subtle lesions of the syndesmosis and deltoid ligament. Three-dimensional (3D) volume measurements by CT in weight bearing reach a sensitivity of 95.8% and a specificity of 83.3% in detecting unstable lesions of the syndesmosis(18).
- Magnetic resonance imaging (MRI): this is the most sensitive test, reaching a sensitivity of 100% and a specificity of 93% in ATFL lesions(19). However, unlike the weight bearing CT scan, MRI has the limitation that it is not always possible to determine with certainty whether the lesion is accompanied by obvious instability of the syndesmosis.
Ankle arthroscopy
Ankle arthroscopy is the gold standard technique for ligament injuries of the ankle. It provides the diagnosis in doubtful cases and is able to define the real extent of the lesion. In addition, it allows the assessment of intraoperative stability.
Arthroscopic evaluation of the syndesmosis
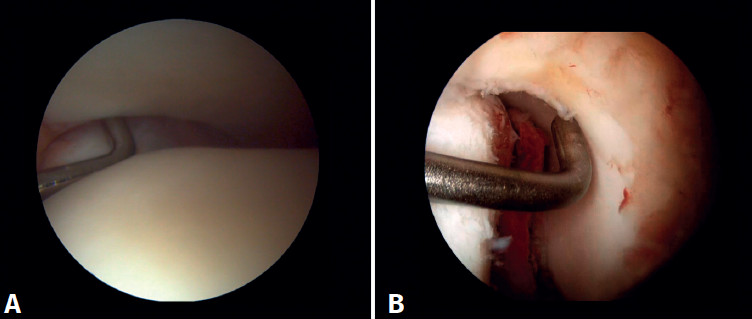
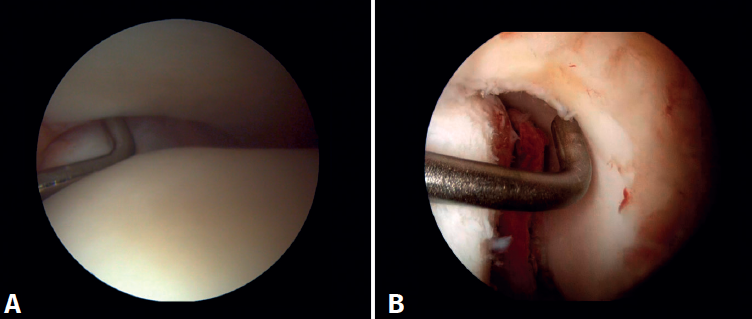
From the anteromedial portal we can directly visualize the distal fibers of the ATFL. Disinsertion of these fibers does not always result in instability of the syndesmosis, but it does require us to check it. In our experience, we prefer assessment of the coronal plane of the syndesmosis. We introduce the arthroscope into the tibiotalar joint directing the camera cranially. In this way we have a direct view of the distal tibiofibular joint. We then assess stability by attempting to insert the palpation probe into the joint. If it is possible to do so, we classify the syndesmosis injury as unstable (Figure 6A).
Arthroscopic evaluation of the deltoid ligament
There are multiple methods for assessing instability of the medial complex; using the anterior ankle portals it is possible to assess the stability of the deltoid ligament in its main plane of action, corresponding to the coronal plane. Chun et al.(20) described instability when it is possible to introduce an arthroscopic palpation probe into the medial tibiotalar space (Figure 6B). Vega et al.(21) reported that, in the majority of injuries, the most anterior portion of the deltoid ligament is detached from the medial malleolus, while its proximal insertions remain intact. In this situation, the arthroscopic palpation probe can be inserted between the medial wall of the internal malleolus and the deep fibers of the deltoid ligament.
Arthroscopic treatment of the syndesmosis and medial complex
Arthroscopic treatment of syndesmosis injuries
There is consensus that a stable injury can be treated on a conservative basis, which includes a period without weight bearing, followed by protected partial weight bearing (with a walking boot) and a rehabilitation protocol(22).
An unstable injury requires surgery to avoid long-term sequelae(23). Ankle arthroscopy remains central to diagnosis and treatment, and it is vital to decide which injuries need to be repaired. Direct visualization of the distal tibiofibular joint is the most accurate way to assess the degree of injury. The association of a deltoid ligament lesion is strongly predictive of an unstable injury.
In addition, up to half of all injuries of the syndesmosis may have concomitant intra-articular disorders (osteochondral lesions or loose bodies)(24), which reinforces the role of arthroscopy for both diagnosis and simultaneous treatment.
It should be noted that injury to the syndesmosis causes disruption of the tibiofibular joint in the coronal and/or sagittal plane. The incidence of joint malreduction when compression clamp reduction is used is 16-52%(25,26). Given these percentages, the use of arthroscopy as a method for controlling reduction is growing in importance.
Surgical technique: arthroscopic treatment of acute syndesmosis injuries
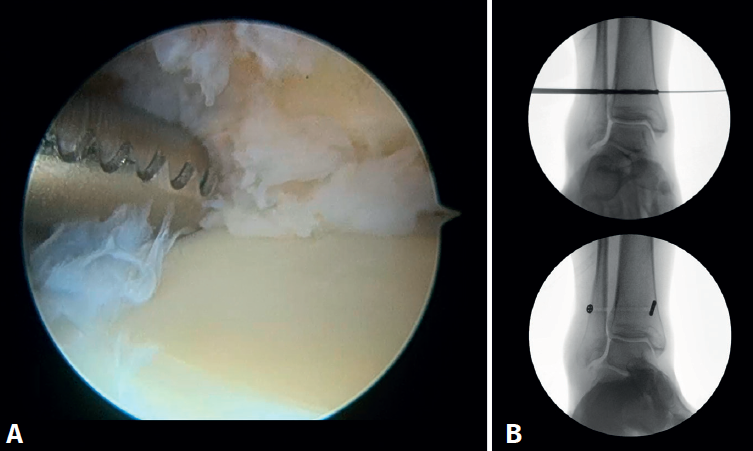
The technique should be performed using the conventional anteromedial and anterolateral portals. The anteromedial portal is used for visualization, while the anterolateral portal serves as the working portal. Once the tibiofibular space is visualized, the inflamed synovial component is resected with an arthroscopic shaver to facilitate reduction (Figure 7A). Then, under direct vision, we restore the tibiofibular space, carefully taking into account possible malrotation of the fibula, especially in Maisonneuve type fractures. For fibular reduction we use a Verbrugge clamp, which allows us to correct the rotation. In our experience, once the space has been cleaned and if the position is correct, it is infrequent to have to use a compression clamp between the tibia and fibula.
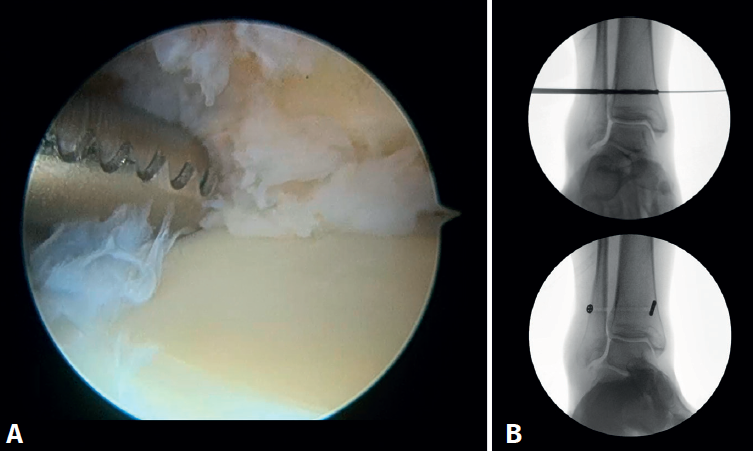
Once the desired reduction has been achieved, we visually check the position and temporarily fix it using a Kirschner pin.
For definitive fixation, the surgical options range between rigid fixation with screws and dynamic fixation. Screws have been the standard procedure for decades, but involve complications, such as loosening or rupture. Furthermore, some surgeons advocate their removal, with the inherent risk of recurrence of instability(27). Dynamic fixation was designed to overcome some of these problems by allowing a degree of physiological movement of the syndesmosis, facilitating early weight bearing, reducing the risk of rupture, and eliminating the need to remove the implant (Figure 7B).
Grassi et al., in a meta-analysis involving over 300 patients, demonstrated an overall decrease in the relative risk of complications (RR = 0.55, p = 0.003) with dynamic systems(28). Raeder et al., in a randomized trial of 97 patients contrasting screw fixation versus a dynamic system, reported a lower incidence of osteoarthritis with suture buttons of 65% versus 35% (p = 0.009) at 5 years(29). Suture button constructions afford a degree of micro-mobility, mimicking physiological mobility, which can promote ligament healing. Likewise, flexible implants are better able to tolerate an imperfect reduction, as a possible complication, even if arthroscopic control of the joint is performed.
Surgical technique: arthroscopic treatment of chronic syndesmosis injuries
Chronic lesions of the syndesmosis are usually underdiagnosed and remain unidentified in a significant percentage of cases. Ankle arthroscopy is an essential tool, with clearly proven efficacy, for the diagnosis and assessment of this type of injury.
The principles referred to fixation are the same, but a more solid option should be chosen, with double screws, double dynamic fixation, or mixed techniques(30,31). Some authors describe techniques involving syndesmosis plasty procedures with autografts (hamstring or peroneus).
Currently, there is insufficient scientific evidence in favor of one surgical technique over another in patients with chronic injuries of the syndesmosis(32,33), and there is a lack of clinical trials to decide which treatment is superior.
The technique used in our practice is the arthroscopic technique without reinforcement plasty. Meticulous arthroscopic debridement of the lower tibiofibular joint is essential to allow complete reduction of the joint. Regarding the type of fixation, we consider that chronic injuries have a higher degree of instability that requires greater fixation, with our preference being the use of a double dynamic system.
Injuries of the medial complex
The deltoid ligament is essential for medial stability of the ankle, as it limits valgus, excessive rotation and anterior translation of the talus. There are usually three main reasons for damage to this ligament: an isolated injury caused by valgus and forced external rotation, associated with chronic lateral instability or in relation to posterior tibial deficiency, producing medial instability as a result(34). Clinically, it presents as anteromedial pain and a feeling of laxity.
The aim of deltoid ligament repair is to reduce external rotation, eversion and anterior translation, since increasing these movements can lead to early osteoarthritis of the ankle(35). In lateral instability in patients with hyperlaxity or severe injury, repair of the anterior portion of the deltoid ligament provides greater fixation to limit anterior translation of the talus(21).
Arthroscopic treatment of medial complex injuries
The deltoid ligament of the ankle can be repaired by open or arthroscopic surgery. While there is ample evidence supporting the safety and efficacy of the open technique(36), comparative studies have emerged in recent years showing similar clinical and radiological results with arthroscopic repair(37). The latter has the advantage of being less aggressive on the soft tissues, which is particularly relevant in trauma patients. It also allows us to simultaneously address other intra-articular lesions.
Surgical technique: arthroscopic treatment of acute medial complex injuries
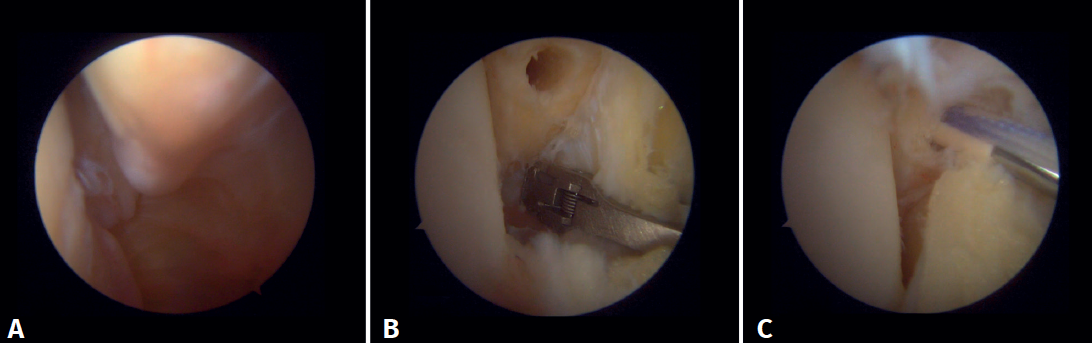
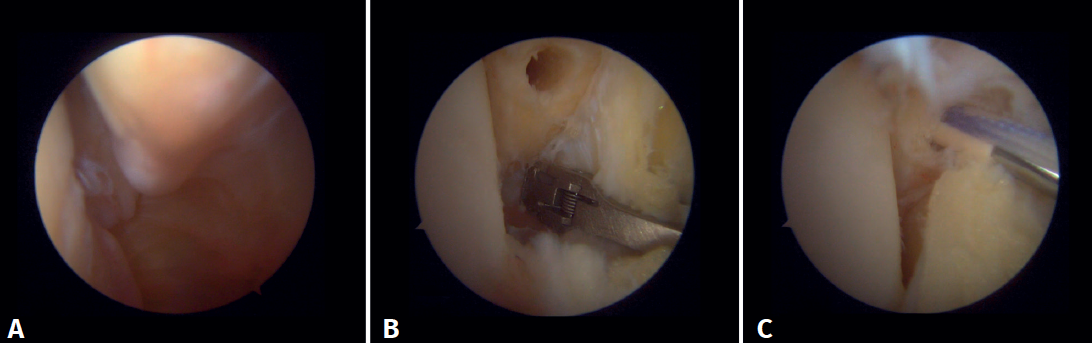
In terms of surgical technique, the working portals are established in the same way as in conventional ankle arthroscopy: one anteromedial portal and one anterolateral portal. We always start with diagnostic arthroscopy to confirm the injury to the deltoid ligament. A probe can be used to verify the laxity of the fibers, and a test can be performed by inserting the probe through the medial groove: the lesion is confirmed if the instrument passes through. For repair, the viewing portal will be the anterolateral portal, thus allowing us to work more directly through the anteromedial portal. The anterior fibers of the superficial tibiotalar and intermediate fibers of the deep portion of the deltoid ligament are the ones that can be repaired with the arthroscopic technique(38). Once the ligament has been identified and dissected, a suture is passed between the fibers using a suture passer. The medial malleolus anchorage zone is prepared with a shaver or a small burr. With the ankle in neutral position, the anchor is inserted while maintaining the tension of the sutures. The intersection of the line parallel to the tibiotalar joint and a perpendicular line marked from the tip of the malleolus and along the lateral border of the malleolus can be used as an anatomical reference for placement(21). After reduction, we again test the fibers for tension and passage of the probe through the medial groove, to confirm adequate repair (Figure 8).
Arthroscopic treatment of chronic medial complex injuries
Ankle arthroscopy is also useful in the treatment of chronic deltoid ligament injuries. Initially, arthroscopy helps to assess the severity of the injury, as well as in treating associated disorders such as osteophytes or cartilage lesions. In severe cases where there is already axial involvement leading to flat foot, additional repair procedures such as correction via calcaneal osteotomy should be considered.
The quality of the ligament with a chronic injury sometimes does not allow repair; in such cases we consider reconstruction performing an autologous graft plasty, e.g., using a gracilis graft or allograft. Loozen et al. recommended reconstruction of both the posterior deep fibers and the anterior tibiotalar fibers, and also added repair to the springligament(36). The results obtained with reconstruction are optimal. However, as Savage-Elliot et al.comment in their article, the repair of a reconstruction is not comparable, since in the latter case there are usually many more associated lesions due to the chronicity of the disorder, and what is intended is mainly to salvage the joint(39).
Conclusions
Ankle arthroscopy is a valuable diagnostic and therapeutic tool for ankle ligament injuries. In the case of the syndesmosis, direct visualization allows accurate assessment of stability, reduces the high incidence of malreduction seen with open techniques, and facilitates the simultaneous treatment of associated intra-articular lesions. In the case of the deltoid ligament, arthroscopy makes it possible to accurately identify the tear, repair the deep fibers and address concomitant injuries, with the advantage of less aggression to the soft tissues - this being particularly relevant in trauma patients.